이 논문은 2003년부터 World Bank에서 Consultant로 일하는 Sara Johansson de Silva 박사와 World Bank에서 Global Lead for Labor & Skills in the Social Protection & Jobs Global Practice로 있는 Indhira Santos 박사가 공동으로 연구하여 발표한 논문입니다.
World Bank (세계은행)은 전세계를 대상으로 한 정책연구를 하는 곳이기 때문에 거시적인 면에서 조사하는 연구논문을 내곤 하는데 전세계적으로 저개발국, 개발도상국 및 선진국을 막론하고 고령화 및 초고령화 사회로 진입하는 것은 사실상 큰 차이가 없는 큰 트렌드입니다.
아래 도표에서는 한국과 모로코, 리베리아가 각각 선진국, 개발도상국 및 저개발국의 표본으로 나왔는데, 저개발국에서는 남녀가 거의 공히 나이가 들어서도 일을 하는 것을 알 수 있습니다.
반면 한국은 남성이 여성에 비해 많이 오래 일하죠. 25-54세 사이에 남성은 90% 정도, 여성은 70% 정도가 일을 하다가 서서히 줄어들어서 65세 이상에서는 남성의 50%, 여성의 30% 정도가 계속 일을 하고 있는 것을 알 수 있습니다.
언론인 손석희가 책 『장면들』에서 가장 중요하게 다루고 있는 것은 ‘어젠다 키핑(agenda keeping)’이다. 어젠다 키핑을 번역하면 ‘의제 지키기’다. 언론의 전통적인 기능 중 하나는 ‘의제 설정’을 뜻하는 ‘어젠다 세팅(agenda setting)’이다. 공론화가 되어 토론할 필요가 있는 사회적 이슈에 카메라와 마이크를 갖다 대는 행위가 바로 어젠다 세팅이다. 어젠다 키핑은 그러한 이슈에 카메라와 마이크를 갖다 대는 시간을 ‘오랫동안 지속하는’ 행위다.
손석희는 “이 책이 주로 다룬 것은 저널리즘의 한 방법론으로서의 ‘어젠다 키핑(agenda keeping)’이다. 이 표현은 내가 주장하긴 했지만 완전히 창의적인 것은 아닐 것”이라며 “그 이전에 의제설정 기능(agenda setting)은 이미 전통적인 미디어 이론으로 널리 알려져 있다. 그러나 미디어가 단지 의제를 세우는 데 그치지 않고, 그 의제를 꾸준히 지켜냄으로써 선한 기여를 할 수 있다는 믿음은 그것과는 좀 다른 얘기”라고 말한다.
손석희가 JTBC의 뉴스 책임자로 어젠다 키핑 개념을 실천한 가장 대표적인 사안은 바로 ‘세월호 참사’였다. 세월호 참사에 대한 언론과 국민들의 관심이 시들고 있을 때에도, JTBC는 참사 이후 200일 동안 쉬지 않고 해당 사안을 지키기 위해 지속적으로 보도했다. 그는 “세월호라는 어젠다를 유지하고 기억하는 것은 의지만 가지고는 안 되는 것이었다”며 “유가족들과 시청자들의 도움과 격려가 없었다면 불가능한 일이었다”고 술회한다
Akriveia Therapeutics LLC, a Thousand Oaks, Calif.-based immuno-oncology focused biotechnology company, raised $7.5m in Series A funding.
The round was led by F-Prime Capital Partners. Thomas Beck and Ben Auspitz of F-Prime Capital Partners will join Akriveia’s Board of Directors in conjunction with the funding. Dr. Beck will become Chairman of the Board.
The company intends to use the funds to expand the team to accelerate its therapeutic discovery efforts, and to build a pipeline of single agent and combination immunotherapeutics.
Led by Chief Executive Officer Simon Tomlinson, Akriveia Therapeutics leverages its proprietary platform to create immunotherapeutic products that are specifically activated in the microenvironment of the tumor. To this end, the company also announced that it has entered into exclusive license agreements for key enabling technologies with City of Hope and Thomas Jefferson University.
Akriveia was founded on the work of Professor John Williams at City of Hope and Professor Ulrich Rodeck at Thomas Jefferson University, experts in the fields of bioengineering and cancer therapeutic discovery.
Akriveia Therapeutics, an emerging immuno-oncology focused biotechnology company, today announced recent key additions to its research leadership team. Dr. C. Glenn Begley has joined the company as Chief Scientific Officer and Dr. Margaret Karow has joined as Vice President of Discovery and Preclinical Development.
Akriveia Therapeutics is harnessing its proprietary platform to create immunotherapeutic products that are specifically activated in the microenvironment of the tumor. It is anticipated that this will substantially increase the utility of immuno-oncology agents and spare patients the treatment-limiting, debilitating and sometimes lethal side-effects of the current generation of immunotherapeutics.
“Glenn and Margaret joining the company are pivotal events for Akriveia,” commented Dr. Simon Tomlinson, Chief Executive Officer of Akriveia Therapeutics, “the depth and breadth of experience in the discovery and development of cancer biologics that they bring to the company is immense. Their expertise will be key to Akriveia rapidly building a proprietary pipeline of next-generation immunotherapeutics. I am thrilled and honored to welcome them to the company.”
Most recently Dr. Begley was Chief Scientific Officer at TetraLogic Pharmaceuticals. For the 10 years prior he was Vice-President and Global Head of Hematology and Oncology Research at Amgen Inc, based in California. His group was responsible for marketed molecules such as Neupogen, Neulasta, Aranesp, Nplate, Xgeva, discovery of 25 new clinical-stage molecules, and in-licensing of molecules such as Imlygic the first approved oncolytic virus therapy and Blincyto, a bi-specific T-cell engager molecule. Dr. Begley’s personal research has focused on hematopoiesis and stem cell biology. He has published over 200 papers that have been highly cited. His recent work includes analysis of the rigor and reproducibility of scientific research. Dr. Begley originally trained in Australia as a medical oncologist and molecular biologist and has received a number of awards including election to the Association of American Physicians in 2008.
Prior to joining Akriveia, Dr. Karow was an Executive Director at Amgen for 10 years. At Amgen, she held multiple roles in drug discovery and development. These included Executive Director in the Biosimilars Business Unit as the lead for Biosimilars Process Development, and as an Executive Director in Discovery Research leading the Biologics Optimization organization, Protein Sciences at the Thousand Oaks campus, and the site head for the Burnaby, Canada research site where XenoMouse antibody development is based. Prior to Amgen, Dr. Karow was at Regeneron Pharmaceuticals for 10 years, where she was the Vice President of Traps, Small Molecule and Antibody Development, and the Immunology therapeutic area. She was also the co-lead for the development of the VelocImmune mouse platform for the production of human antibodies. As a leader in biotechnology, she has shepherded multiple large molecule projects from their discovery stage and into clinical trials, as well as to the successful filing of marketing applications. Margaret completed her post-doctoral work at Temple Medical School and her Ph.D. at the University of Utah, and holds a BA in MCD Biology from the University of Colorado.
“I’m excited to be joining Akriveia at this strategic stage of its development,” noted Dr. Begley, “the scientific founders have built a powerful and novel platform for the discovery of immuno-therapeutics with pharmacological action targeted to tumor sites. I’m looking forward to helping the company drive the development of a proprietary pipeline and to exploring partnerships that combine our strengths with those of other pharma and biotechnology companies.”
“Akriveia presented a unique opportunity for me to apply my experience of biotherapeutic discovery and development at an early stage company in the immuno-oncology field,” noted Dr. Karow, “the Akriveia approach offers the promise of tackling a significant unmet medical need for safer and more effective immuno-oncology agents. I’m delighted to have joined Akriveia and I am looking forward to helping the company build a pipeline of innovative immunotherapeutics.”
About Akriveia Therapeutics
Akriveia Therapeutics is actively pursuing the discovery and development of the next generation of cancer immunotherapies. Akriveia believes its new agents offer the promise of a safer and more efficacious approach to harness a patient’s own immune system to fight cancer. Akriveia was founded on the pioneering work of Professor John Williams at City of Hope and Professor Ulrich Rodeck at Thomas Jefferson University, experts in the fields of bioengineering and cancer therapeutic discovery. The company is backed by leading life science investor FPrime Capital Partners.
Akriveia Therapeutics, an immuno-oncology focused biotechnology company, today announced its Aklusion™ platform for tumor-targeting cancer immunotherapies will be featured in a poster presentation at the Society for Immunotherapy of Cancer’s (SITC) 32nd Annual Meeting, November 10-12, 2017, at Gaylord National Hotel & Convention Center in National Harbor, MD.
The poster’s authors include scientists from the laboratories of Professor John Williams of the Beckman Research Institute at the City of Hope and Professor Ulrich Rodeck at Thomas Jefferson University, along with Dr. Margaret Karow, Senior Vice President of Drug Discovery and Preclinical Development at Akriveia Therapeutics.
Information about the poster presentation is:
Poster Title: Rational Design of Immuno-Oncology Biologics with Improved Safety and Efficacy
Poster Number: P466
Poster Session: Saturday November 11th 12:30pm-2:00pm and 6:30pm-8:00pm
Akrevia Therapeutics, a privately-held biopharmaceutical company focused on developing highly-potent, tumor-targeted immuno-oncology therapeutics, today announced the closing of a $30 million Series A financing led by F-Prime Capital Partners and Atlas Venture. The investors have come together to recruit an experienced management team to accelerate Akrevia’s pipeline and proprietary Aklusion® platform, which allows therapeutic antibodies, cytokines and chemokines to be specifically activated in the tumor microenvironment and tailored with precisely optimized pharmacologic properties.
Akrevia will be led by Tim Clackson, Ph.D., as President and Head of R&D and Nessan Bermingham, Ph.D., as Executive Chairman. Dr. Clackson joins Akrevia after serving as President of R&D at ARIAD Pharmaceuticals, where he led the discovery and development of Iclusig® (ponatinib) and Alunbrig® (brigatinib), two FDA-approved cancer therapeutics. Dr. Bermingham was most recently CEO of Intellia Therapeutics, a leading gene editing company which he founded, built, and took public.
“We are excited to have the opportunity to work with Tim and Nessan, two experienced drug developers and entrepreneurs who have helped deliver novel therapies to patients and built successful, billion-dollar biotechs,” said Ben Auspitz, F-Prime Capital Partners.
“We were attracted by the strong validation of Akrevia’s founding technology from City of Hope, and the opportunity to harness the therapeutic potential of cytokines and chemokines,” said David Grayzel, M.D., Atlas Venture. “We believe that the Akrevia team and platform will unlock the potential of multiple important immuno-oncology mechanisms and deliver a pipeline of potent, targeted agents to patients.”
Optimizing Potency and Delivery: Aklusion Platform Technology
Akrevia’s Aklusion platform, based on technology licensed from City of Hope and Thomas Jefferson University, allows potently active biological molecules to be inactive until they encounter the tumor microenvironment. With a potential best-in-class anti-CTLA4 antibody as validation, the technology can be applied broadly to other biologic architectures, including highly-potent cytokines and chemokines which currently have limited or no clinical utility due to toxicities. By tailoring pharmacokinetic and pharmacodynamic properties in parallel, Aklusion allows design of molecules with potential best-in-class potency and selectivity.
“Targeting is key to unlocking the true potential of immuno-oncology,” said Tim Clackson, Ph.D., President and EVP R&D, Akrevia Therapeutics. “Currently, we don’t lack potential agents – just the ability to effectively and safely deliver them where they’re needed, and with precisely tailored properties. Our vision at Akrevia is to unleash the full potential of immune stimulating molecules including antibodies, cytokines and chemokines, as new options for patients living with cancer.”
Additional Akrevia leadership includes Ronan O’Hagan, Ph.D., who formerly co-led the oncology discovery program at Merck, as SVP of Discovery, and Margaret Karow, Ph.D., formerly of Amgen and Regeneron, as SVP of Preclinical Development. Thomas Beck, M.D., and Ben Auspitz of F-Prime Capital serve on the Board of Directors alongside David Grayzel, M.D. and Michael Gladstone of Atlas Venture.
About Akrevia Therapeutics
Akrevia Therapeutics, LLC is a privately-held biopharmaceutical company focused on developing highly-potent, targeted immuno-oncology therapeutics. The company’s proprietary Aklusion platform technology allows biologics to be specifically activated in the tumor microenvironment, and with precisely tailored properties, expanding the universe of immune-activating proteins that can be safely delivered. Akrevia is applying its technology to build a broad pipeline of engineered antibodies, cytokines and chemokines as potential new options for patients living with cancer. To learn more, please visit www.akrevia.com.
Xilio Therapeutics, a company developing potent, tumor-selective immuno-oncology (IO) therapies for patients with cancer, today announced the closing of a $100.5 million Series B financing. Proceeds from the financing will be used to progress Xilio’s first two therapeutic candidates, XTX201 (tumor-selective IL-2) and XTX101 (tumor-selective aCTLA4 mAb) through Investigational New Drug (IND) enabling studies and into Phase 1 clinical trials, as well as advance additional tumor-selective cytokine programs using Xilio’s proprietary technology.
The financing was led by Takeda Ventures, Inc. with new investors SV Health Investors, MRL Ventures Fund, RiverVest Venture Partners, Bay City Capital, Solasta Ventures, M Ventures, and Ipsen Ventures joining existing investors F-Prime Capital and Atlas Venture in the syndicate.
“We are fortunate to have the support of investors who share our vision to deliver highly potent and effective tumor-selective cancer therapies to patients,” said Rene Russo, Chief Executive Officer of Xilio Therapeutics. “This is a transformational moment for the company as we work to bring our first development programs to patients with cancer and expand our tumor-selective cytokine pipeline.”
Xilio Therapeutics is developing its proprietary technology to create a new class of ultra-potent IO therapies that are activated selectively within the tumor. These tumor-selective therapies are designed to overcome the significant toxicities associated with validated IO therapies, such as IL-2 and aCTLA4, which have historically limited the number of patients that can be treated and prevented patients from completing full courses of treatment. XTX201 (IL-2) and XTX101 (aCTLA4 mAb) have demonstrated tumor-selective activity in preclinical models, significantly widening the potential therapeutic index for these therapies.
“IO has emerged as a major driver of cancer therapeutic development, and agents in this space have proven effective, resulting in compelling durable clinical responses,” stated Jayson Punwani, Investment Partner with Takeda Ventures. “We believe Xilio’s proprietary platform offers a compelling approach that builds upon the advancements in IO therapeutics. It is encouraging to see such a strong and supportive Series B syndicate, including leading venture capital groups and strategic partners. We look forward to working with Xilio’s current investors and the leadership team to support the advancement of its pipeline into the clinic.”
In connection with the closing of the financing, Mr. Punwani, Mike Ross of SV Health Investors, Peter Dudek of MRL Ventures Fund (the therapeutics-focused venture capital group within Merck), and Nancy Hong of RiverVest Venture Partners each joined the Board of Directors of Xilio.
The rebranding of the company from Akrevia Therapeutics to Xilio Therapeutics (pronounced “ex-il-ee-oh”) reflects the company’s evolution from a research-focused organization to a development stage company and commitment to developing the next generation of ultra-potent IO therapies. Xilio is derived from the Latin term Ex Nihilo, meaning creation or big-bang, and embodies the company’s vision to create the next generation of transformative cancer treatments for individuals living with cancer by unleashing the full power of highly potent immune therapies precisely in tumors.
About Xilio Therapeutics Xilio Therapeutics is a biotechnology company advancing next-generation cancer immunotherapies designed to improve patient outcomes by unleashing the power of the immune system selectively at the site of the tumor. The company’s tumor-selective immunotherapies are based on its proprietary technology, which maximizes the potency of proven immuno-oncology therapies and restricts their activity to the tumor to minimize peripheral side effects. The broad applicability of these therapies across cancer types means that all patients could benefit from these potentially curative medicines.
Xilio was founded in 2016 and is headquartered in Waltham, Mass. For more information, please visit www.xiliotx.com
Xilio Therapeutics has raised $95 million to take IL-2 and CTLA-4 immunotherapies into clinical trials. The series C positions Xilio to provide early clinical validation of anti-cancer agents that are designed to remain inactive until they reach tumors.
Immuno-oncology drugs are typically given systemically, causing them to trigger immune responses that affect healthy and cancerous tissues alike. The resulting adverse events are unpleasant and can prevent physicians from administering the most efficacious dose. Patients suffer from both the side effects and worse outcomes due to the use of suboptimal doses.
Xilio, formerly known as Akrevia Therapeutics, is built on a platform designed to minimize the effect of cancer drugs on healthy tissues. The potential of the platform has attracted a who’s who of VCs.
Rock Springs Capital led the series C round with support from new backers including Bain Capital Life Sciences, Deerfield Management and RA Capital Management. Existing Xilio investors including Atlas Venture, SV Health Investors and Takeda Ventures also contributed to the financing.
Xilio will use the money to take two drugs, XTX202 and XTX101, into clinical development. XTX202 is a formulation of IL-2, a cytokine that is hamstrung by limitations such as a short half-life and immune effects that necessitate the administration of high doses. XTX101 is a monoclonal antibody against CTLA-4, the immune checkpoint receptor targeted by Bristol Myers Squibb’s Yervoy. INDs for both candidates are planned for this year.
Working with technology licensed from City of Hope and Thomas Jefferson University, Xilio links the drugs to peptides designed to mask the molecules until they reach the tumor microenvironment. The linker is cleaved by proteases found near to tumors, causing the targeted unmasking of the drug.
The approach holds particular promise for potentially highly efficacious molecules that must be given at reduced doses due for safety and tolerability reasons. Xilio thinks IL-2 and CTLA-4 fit the bill.
“While high dose rhIL-2 has the potential for durable complete responses, it is only given to a small number of patients due to its life-threatening toxicity. Similarly, approved aCTLA4 therapy produces severe autoimmune toxicity, limiting potential benefit by preventing patients from receiving highly therapeutic doses or completing full courses of treatment,” Martin Huber, M.D., Xilio chief medical officer, said in a statement.
Xilio Therapeutics, Inc. (Xilio) a biotechnology company developing tumor-selective immuno-oncology therapies for patients with cancer, today announced the closing of its previously announced initial public offering of 7,353,000 shares of its common stock at a price to the public of $16.00 per share. The aggregate gross proceeds to Xilio from the offering were approximately $117.6 million, before deducting underwriting discounts and commissions and estimated offering expenses payable by Xilio. In addition, Xilio has granted the underwriters a 30-day option to purchase up to an additional 1,102,950 shares of its common stock at the initial public offering price less underwriting discounts and commissions.
The shares began trading on the Nasdaq Global Select Market on October 22, 2021 under the ticker symbol “XLO.”
Morgan Stanley, Cowen and Guggenheim Securities acted as joint book-running managers for the offering. Raymond James acted as lead manager for the offering.
Gilead Sciences is bucking the trend in IL-12, handing Xilio Therapeutics $43.5 million upfront to get into the space after seeing rivals such as AstraZeneca and Bristol Myers Squibb retreat from the cytokine. Xilio shared the news alongside details of plans to pull back from another program and lay off 21% of its staff.
The Xilio deal gives Gilead a global license to develop and commercialize XTX301, Xilio’s tumor-activated IL-12. Like its sibling IL-2, the cytokine is a potentially potent immunotherapy, but efforts to realize that promise have repeatedly run into setbacks. Drug developers have come up with a range of ways to try to address the toxicity and half-life problems but are yet to deliver an approved IL-12 product.
Xilio’s attempt to crack the challenge rests on the addition of domains for masking and half-life extension to IL-12. Coupled to the domains, IL-12 could travel harmlessly around the body until it enters the tumor microenvironment, where an enzyme removes both add-ons and thereby activates the cytokine.
The biotech is putting that idea to the test in a phase 1 clinical trial. Patients with advanced solid tumors are receiving XTX301 every three weeks. In January, the biotech told investors the drug was generally well tolerated into the third dose level, with no dose-limiting toxicities, and committed to providing safety, pharmacokinetic and pharmacodynamic data in the second half of 2024.
Gilead has made its move ahead of the data drop, handing Xilio $30 million in cash and investing $13.5 million in the biotech in return for an exclusive global license. Xilio is responsible for running the phase 1 trial through dose escalation. Once Gilead receives the data package, it can choose to pay $75 million to take responsibility for further development.
By the time Gilead makes that decision, Xilio could have received up to $29 million more from the Big Biotech in the form of additional equity investments and a development milestone payment. The fees are part of a package of milestones and investments worth up to $604 million. Shares in Xilio, which have languished below $1 this year, shot up by more than 200% in the wake of the update to exceed $2.
The agreement moves Gilead into a space that some of its peers have entered and exited in recent years. Across two updates in 2022 and 2023, AstraZeneca dropped a Moderna-partnered mRNA prospect that encodes for IL-12 and axed an oncolytic viral agent engineered to include a transgene-encoding IL-12. In between those events, BMS returned the rights to Dragonfly Therapeutics’ IL-12 therapy.
Gilead is poised to take the baton from Xilio and carry XTX301 through the rest of the race against those rivals. The transfer will leave Xilio focused on its CTLA-4 prospect XTX101, phase 2 data on which are due later this year. Xilio has a third clinical-phase asset, the IL-2 candidate XTX202, but it has decided to stop investing in monotherapy development.
Xilio disclosed the decision alongside new phase 2 data on XTX202 in patients with kidney cancer and melanoma. Stable disease continued to be the best response, leading the biotech to “explore strategic opportunities” for further development in combinations. With its focus narrowing, Xilio is parting ways with 15 employees, representing a 21% reduction of its workforce.
SINGAPORE — Rosalind Tay left her job in April after she reached Singapore’s retirement age of 62, but she was far from ready to call it a career.
“I assume I will be living until 90-plus, like my parents, so I cannot survive based on my current savings,” said the former employee of a baby milk formula company. She said that medical bills are expensive, she wants to travel more, and she hopes to stay active to ward off dementia and other chronic diseases.
“I want to work as long as my body can.”
Singapore and other aging Asian societies are beginning to adjust their labor systems to accommodate people like Tay — and keep their own public welfare burdens in check. The city-state and governments across the region have started discussions on raising the age at which workers are expected, or in some cases required, to retire, delaying the start of pension payouts. But tapping the potential of senior workers is likely to take a lot more than just changing a number.
Singapore’s citizens and permanent residents aged 65 or older accounted for 13.7% of the population as of June 2018, up from 8.7% in 2008, making it one of the fastest-graying countries in Asia. People are also living longer: Singapore’s average life span in 2040 is expected to be 85.4 years, third-highest after Spain (85.8) and Japan (85.7), according to a study last year by the Institute for Health Metrics and Evaluation in the U.S.
In an interview with the Nikkei Asian Review in May, Singaporean Deputy Prime Minister Heng Swee Keat posed a key question his government is facing: “If our people are living longer, how do we create a structure that will enable them to continue to work if they wish to work?”
He said the city-state needs to deal with demographic changes to achieve what it calls “productive longevity.”
One challenge is to ensure seniors have the skills they need. Tay is enrolled in a program offered by the nonprofit Center For Seniors, where participants — mostly in their 50s and 60s — get a refresher course in preparing for job interviews and tips on maintaining motivation. “I learned the importance of being open, confident and willing to learn,” Tay said after a CFS seminar in early June. An average of 3,000 people attend various CFS programs each year.
Increasing the number of seniors in the workforce is seen as a crucial step toward shoring up Asian countries’ labor pools.
Singaporeans attend a job seminar organized by the Center For Seniors on June 10. (Photo by Kentaro Iwamoto)
“Raising the retirement age is an urgent matter to prevent a labor shortage as a result of an aging population,” said Doan Mau Diep, a deputy minister in Vietnam’s Ministry of Labor – Invalids and Social Affairs.
Hanoi plans to raise the retirement age to 62 for men and 60 for women, from the current 60 and 55, based on a proposal to the national assembly earlier this year.
Vietnam’s working-age population is decreasing and its dependence ratio is rising, the authorities say. Official statistics show that only 2 million people entered the workforce in the five years to 2018; fifteen years ago, 1.2 million were joining every year. The unemployment rate remained just 2% in 2018.
At the same time, the average life span has increased to 71.1 years for men and 81.3 years for women.
Thailand is grappling with similar issues. The country’s central bank says the aging population is likely to slow gross domestic product growth by 1.5 percentage points over the next decade.
“On average, the country’s GDP growth was around 5% per annum for the past 10 years,” said Don Nakornthab, senior director of the Bank of Thailand’s economic and policy department. “As society ages and the workforce shrinks, Thailand’s GDP growth could be at 3.5% annually over the next decade if this structural problem remains unsolved.” Active seniors are arguably becoming as important as robots and automation in keeping Southeast Asia’s second-largest economy running.
On May 21, Prime Minister Prayuth Chan-ocha’s previous junta cabinet approved a move to extend the retirement age for civil servants who will reach the current threshold of 60 in the next fiscal year. By how much is a question left for his current government.
This has sparked an intense debate among bureaucrats and intellectuals. The Office of the Civil Service Commission has suggested a new retirement age of 63. The Thailand Development Research Institute would like to see it raised to 65 in both the public and private sectors.
As for Japan, the world leader in aging, Prime Minister Shinzo Abe on June 5 unveiled a draft update to his economic growth strategy. One of the new initiatives is to push companies to let employees work until 70.
The government wants large corporations to do more to carry the burden of the aging society and swelling pension outlays. Companies are beginning to relent: The four biggest steelmakers in April announced they would raise their retirement age to 65 from 60 in 2021.
Nippon Steel said it is “doing its part” to help Japan overcome the pension crisis and aging population.
Company officials also noted that, although steelmaking is now largely automated, it still requires human skills and they need older workers to pass on their knowledge. The industry has about 200,000 workers in Japan, and its decision could prompt other manufacturers to follow suit.
When it comes to China — the only country with more than 200 million seniors — many experts have called for raising the official retirement age beyond 60. Beijing faces the dual challenges of an aging population and declining births, which can cause governments to fall behind on pension payouts.
Still, while policymakers are eager to get more seniors working and some companies see the wisdom of it, not all employees and employers are happy about pushing back retirement.
The Japanese government wants large corporations to do more to carry the burden of the aging society and swelling pension outlays. (Photo by Hideki Yoshikawa)
Pham Quynh Tran, a 45-year-old worker at a confectionery company in Vietnam’s southern Dongnai Province, has been on the job for 25 years and thinks another 10 is enough. “Extending the working age is only suitable for those who work in special fields, such as education or research,” she said. “I don’t think the health condition is good for workers at factories like me.”
Tran is skeptical about the shortage argument, since 100,000 Vietnamese go overseas every year as part of a labor export program. “Only officials who work for an authority or the government and get many perks are happy with the retirement age proposal,” she said.
Likewise, the head of a cosmetics company in Ho Chi Minh City who spoke on condition of anonymity said he is concerned about the plan. He said his company needs younger workers and the change would increase labor costs. If the proposal is approved, he fears he will have to restructure the company’s salary and reward systems, as well as relocate many older employees.
The yearning for youth is still strong in corporate Japan, too. “Many executives think older workers tend to be less amenable and harder to work with,” said Hideki Oe, a former Nomura banker and retirement consultant. “The truth is companies want to hire young people if it’s possible.”
Most Japanese companies continue to provide some work for employees after they retire at 60. Employers with a retirement age of 65 are still a minority and tend to be concentrated in labor-intensive industries, such as health care, restaurants, hotels, construction and delivery, data from the labor ministry shows.
The Philippines, for its part, is bucking the trend toward delaying retirement. The House of Representatives recently approved a measure allowing government workers to retire at 56 if they so choose — rather than 60 — and still receive full benefits. “To those who do not want to serve anymore, government employees can retire earlier,” Representative Antonio Tinio, the lead proponent, said. “It will be better for morale as a whole.”
Elsewhere, though, the reality is that policymakers, employers and workers are all under pressure to adjust to changing demographics. As people work longer, they will need an array of social systems in place, from education to keep up with new technologies to infrastructure upgrades — especially in less developed countries — that ensure it is safe and easy for older individuals to commute.
In many Asian countries, “older people did not have a lot of education [when they were young],” according to Thang Leng Leng, an associate professor at the National University of Singapore. She pointed out that re-education and retraining are crucial for societies to bring more seniors into the workforce and ensure they are productive.
Thang said governments also need to consider seniors’ work-life balance if they want them to put off retirement. “A lot of people don’t mind working, but they don’t want to work all the time,” she said. “In trying to get people to work longer, there’s really a need to restructure work.”
Beh Swan Gin, chairman of Singapore’s Economic Development Board, told the Nikkei Asian Review, “We have to re-imagine how we can create an economy where [seniors] can productively contribute.”
He said the government should raise the retirement age “at a pace where employers are able to cope,” since it will take time to change their focus on recruiting young people.
“How do you have this workforce where you have very different generations, all [with] different needs?” Beh said. “How do you combine that so that [your] operations do even better? It is a journey we all have to go through.”
Henry Quake, an adviser at the Center For Seniors in Singapore, said it is important for societies to help older citizens make the most of their talents. “The senior,” he said, “is a gold mine.”
Nikkei staff writers Mitsuru Obe in Tokyo, Masayuki Yuda in Bangkok and Mikhail Flores in Manila contributed to this story.
Productive Longevity 에 대해 얘기한 분으로 Peter F. Drucker 교수님이 계십니다. Drucker 교수님은 University of Pennsylvania에서 경영학 교수로서 기업경영이란 불모의 영역을 개척하신 분일 뿐만 아니라 자신 스스로 “Productive Longevity (의미있게 오래살기)”를 사신 분으로 미국에서는 Role Model로 여겨지십니다. 96세 생일을 8일 남기고 세상을 떠나실 때까지 쉬지 않고 집필 및 비영리기관을 돕는 일을 하시고 소위 “Social Entrepreneur (사회적 기업가)”의 원조가 되신 분이십니다. Drucker 교수님께서 돌아가시기 6년전인 1999년 (90세) 에 Harvard Business Review에 쓰신 글이 있어서 나누며 생각해 보고자 합니다.
Feedback Analysis”를 통해 나의 강점을 찾을 수 있다. 중요한 결정을 내릴 때마다 무엇을 기대하는지 적어두고 9-12개월 후에 기대했던 것과 실제로 얻은 결과를 비교해 보라.
Feedback Analysis를 계속하면 2-3년 이내에 나의 강점을 알게 되는데 이것이 가장 중요한 지식이다. 이 결과로 부터 할 것은 첫째, 강점에 집중하는 것이다. 자신이 강점이 있는 분야에서 노력할 때 결과를 얻을 수 있다. 둘째 강점을 계발하기 위해 노력하라.
셋째, 지적교만으로 인해 배워야할 것을 배우지 못하는 우를 범하지 말라. 나의 강점을 최대로 실현하기 위해서 배워야 할 기술이나 지식이 있다면 그것을 배워야 한다.
일을 효과적으로 성취할 수 없게 만드는 나쁜 습관을 치료하라. Feedback을 통해 문제의 원인이 매너 부족때문이라는 것을 알게 될수도 있다. 기대와 실제 결과를 비교하다 보면 하지 말아야 할 것을 찾을 수 있게 된다. 약점은 무시하고 모든 에너지와 시간을 오로지 강점에 집중해야만 유능한 사람을 스타로 만들 수 있다.
어떻게 배우고 성과를 내는가?
이것은 개인성향의 문제여서 바꿀 수 없다. 나는 글을 통해 배우는가? 아니면 들어서 배우는가? 나는 사람들과 함께 일을 잘하는가? 아니면 혼자일 때 일을 잘하는가? 어떤 사람들은 팀멤버로서 일을 잘하고 어떤 사람들은 혼자일 때 일을 잘한다. 나는 결정권자일 때 결과를 내는가 아니면 조언자일 때 결과를 내는가? 대다수는 훌륭한 조력자이지만 결정을 내려야 하는 부담과 압력을 견디지 못한다. 나는 쫓기는 상황일 때 일을 잘하는가 아니면 미리 준비된 상황에서 일을 잘하는가? 나는 큰 조직에서 일을 잘하는가 아니면 작은 조직에서 일을 잘하는가? – 이것을 아는 것이 중요하다.
Summary.
Throughout history, people had little need to manage their careers—they were born into their stations in life or, in the recent past, they relied on their companies to chart their career paths. But times have drastically changed. Today we must all learn to manage ourselves.
What does that mean? As Peter Drucker tells us in this seminal article first published in 1999, it means we have to learn to develop ourselves. We have to place ourselves where we can make the greatest contribution to our organizations and communities. And we have to stay mentally alert and engaged during a 50-year working life, which means knowing how and when to change the work we do.
It may seem obvious that people achieve results by doing what they are good at and by working in ways that fit their abilities. But, Drucker says, very few people actually know—let alone take advantage of—their fundamental strengths.
He challenges each of us to ask ourselves: What are my strengths? How do I perform? What are my values? Where do I belong? What should my contribution be? Don’t try to change yourself, Drucker cautions. Instead, concentrate on improving the skills you have and accepting assignments that are tailored to your individual way of working. If you do that, you can transform yourself from an ordinary worker into an outstanding performer.
Today’s successful careers are not planned out in advance. They develop when people are prepared for opportunities because they have asked themselves those questions and have rigorously assessed their unique characteristics. This article challenges readers to take responsibility for managing their futures, both in and out of the office.close
History’s great achievers—a Napoléon, a da Vinci, a Mozart—have always managed themselves. That, in large measure, is what makes them great achievers. But they are rare exceptions, so unusual both in their talents and their accomplishments as to be considered outside the boundaries of ordinary human existence. Now, most of us, even those of us with modest endowments, will have to learn to manage ourselves. We will have to learn to develop ourselves. We will have to place ourselves where we can make the greatest contribution. And we will have to stay mentally alert and engaged during a 50-year working life, which means knowing how and when to change the work we do.
What Are My Strengths?
Most people think they know what they are good at. They are usually wrong. More often, people know what they are not good at—and even then more people are wrong than right. And yet, a person can perform only from strength. One cannot build performance on weaknesses, let alone on something one cannot do at all.
Throughout history, people had little need to know their strengths. A person was born into a position and a line of work: The peasant’s son would also be a peasant; the artisan’s daughter, an artisan’s wife; and so on. But now people have choices. We need to know our strengths in order to know where we belong.
The only way to discover your strengths is through feedback analysis. Whenever you make a key decision or take a key action, write down what you expect will happen. Nine or 12 months later, compare the actual results with your expectations. I have been practicing this method for 15 to 20 years now, and every time I do it, I am surprised. The feedback analysis showed me, for instance—and to my great surprise—that I have an intuitive understanding of technical people, whether they are engineers or accountants or market researchers. It also showed me that I don’t really resonate with generalists.
Feedback analysis is by no means new. It was invented sometime in the 14th century by an otherwise totally obscure German theologian and picked up quite independently, some 150 years later, by John Calvin and Ignatius of Loyola, each of who incorporated it into the practice of his followers. In fact, the steadfast focus on performance and results that this habit produces explains why the institutions these two men founded, the Calvinist church and the Jesuit order, came to dominate Europe within 30 years.
Practiced consistently, this simple method will show you within a fairly short period of time, maybe two or three years, where your strengths lie—and this is the most important thing to know. The method will show you what you are doing or failing to do that deprives you of the full benefits of your strengths. It will show you where you are not particularly competent. And finally, it will show you where you have no strengths and cannot perform.
Several implications for action follow from feedback analysis. First and foremost, concentrate on your strengths. Put yourself where your strengths can produce results.
Second, work on improving your strengths. Analysis will rapidly show where you need to improve skills or acquire new ones. It will also show the gaps in your knowledge—and those can usually be filled. Mathematicians are born, but everyone can learn trigonometry.
Third, discover where your intellectual arrogance is causing disabling ignorance and overcome it. Far too many people—especially people with great expertise in one area—are contemptuous of knowledge in other areas or believe that being bright is a substitute for knowledge. First-rate engineers, for instance, tend to take pride in not knowing anything about people. Human beings, they believe, are much too disorderly for the good engineering mind. Human resources professionals, by contrast, often pride themselves on their ignorance of elementary accounting or of quantitative methods altogether. But taking pride in such ignorance is self-defeating. Go to work on acquiring the skills and knowledge you need to fully realize your strengths.
It takes far more energy to improve from incompetence to mediocrity than to improve from first-rate performance to excellence.
It is equally essential to remedy your bad habits—the things you do or fail to do that inhibit your effectiveness and performance. Such habits will quickly show up in the feedback. For example, a planner may find that his beautiful plans fail because he does not follow through on them. Like so many brilliant people, he believes that ideas move mountains. But bulldozers move mountains; ideas show where the bulldozers should go to work. This planner will have to learn that the work does not stop when the plan is completed. He must find people to carry out the plan and explain it to them. He must adapt and change it as he puts it into action. And finally, he must decide when to stop pushing the plan.
At the same time, feedback will also reveal when the problem is a lack of manners. Manners are the lubricating oil of an organization. It is a law of nature that two moving bodies in contact with each other create friction. This is as true for human beings as it is for inanimate objects. Manners—simple things like saying “please” and “thank you” and knowing a person’s name or asking after her family—enable two people to work together whether they like each other or not. Bright people, especially bright young people, often do not understand this. If analysis shows that someone’s brilliant work fails again and again as soon as cooperation from others is required, it probably indicates a lack of courtesy—that is, a lack of manners.
Comparing your expectations with your results also indicates what not to do. We all have a vast number of areas in which we have no talent or skill and little chance of becoming even mediocre. In those areas a person—and especially a knowledge worker—should not take on work, jobs, and assignments. One should waste as little effort as possible on improving areas of low competence. It takes far more energy and work to improve from incompetence to mediocrity than it takes to improve from first-rate performance to excellence. And yet most people—especially most teachers and most organizations—concentrate on making incompetent performers into mediocre ones. Energy, resources, and time should go instead to making a competent person into a star performer.
How Do I Perform?
Amazingly few people know how they get things done. Indeed, most of us do not even know that different people work and perform differently. Too many people work in ways that are not their ways, and that almost guarantees nonperformance. For knowledge workers, How do I perform? may be an even more important question than What are my strengths?
Like one’s strengths, how one performs is unique. It is a matter of personality. Whether personality be a matter of nature or nurture, it surely is formed long before a person goes to work. And how a person performs is a given, just as what a person is good at or not good at is a given. A person’s way of performing can be slightly modified, but it is unlikely to be completely changed—and certainly not easily. Just as people achieve results by doing what they are good at, they also achieve results by working in ways that they best perform. A few common personality traits usually determine how a person performs.
Am I a reader or a listener?
The first thing to know is whether you are a reader or a listener. Far too few people even know that there are readers and listeners and that people are rarely both. Even fewer know which of the two they themselves are. But some examples will show how damaging such ignorance can be.
When Dwight Eisenhower was Supreme Commander of the Allied forces in Europe, he was the darling of the press. His press conferences were famous for their style—General Eisenhower showed total command of whatever question he was asked, and he was able to describe a situation and explain a policy in two or three beautifully polished and elegant sentences. Ten years later, the same journalists who had been his admirers held President Eisenhower in open contempt. He never addressed the questions, they complained, but rambled on endlessly about something else. And they constantly ridiculed him for butchering the King’s English in incoherent and ungrammatical answers.
Eisenhower apparently did not know that he was a reader, not a listener. When he was Supreme Commander in Europe, his aides made sure that every question from the press was presented in writing at least half an hour before a conference was to begin. And then Eisenhower was in total command. When he became president, he succeeded two listeners, Franklin D. Roosevelt and Harry Truman. Both men knew themselves to be listeners and both enjoyed free-for-all press conferences. Eisenhower may have felt that he had to do what his two predecessors had done. As a result, he never even heard the questions journalists asked. And Eisenhower is not even an extreme case of a nonlistener.
A few years later, Lyndon Johnson destroyed his presidency, in large measure, by not knowing that he was a listener. His predecessor, John Kennedy, was a reader who had assembled a brilliant group of writers as his assistants, making sure that they wrote to him before discussing their memos in person. Johnson kept these people on his staff—and they kept on writing. He never, apparently, understood one word of what they wrote. Yet as a senator, Johnson had been superb; for parliamentarians have to be, above all, listeners.
Few listeners can be made, or can make themselves, into competent readers—and vice versa. The listener who tries to be a reader will, therefore, suffer the fate of Lyndon Johnson, whereas the reader who tries to be a listener will suffer the fate of Dwight Eisenhower. They will not perform or achieve.
How do I learn?
The second thing to know about how one performs is to know how one learns. Many first-class writers—Winston Churchill is but one example—do poorly in school. They tend to remember their schooling as pure torture. Yet few of their classmates remember it the same way. They may not have enjoyed the school very much, but the worst they suffered was boredom. The explanation is that writers do not, as a rule, learn by listening and reading. They learn by writing. Because schools do not allow them to learn this way, they get poor grades.
Schools everywhere are organized on the assumption that there is only one right way to learn and that it is the same way for everybody. But to be forced to learn the way a school teaches is sheer hell for students who learn differently. Indeed, there are probably half a dozen different ways to learn.
A chief executive I know who converted a small and mediocre family business into the leading company in its industry was one of those people who learn by talking. He was in the habit of calling his entire senior staff into his office once a week and then talking at them for two or three hours. He would raise policy issues and argue three different positions on each one. He rarely asked his associates for comments or questions; he simply needed an audience to hear himself talk. That’s how he learned. And although he is a fairly extreme case, learning through talking is by no means an unusual method. Successful trial lawyers learn the same way, as do many medical diagnosticians (and so do I).
There are people, like Churchill, who learn by writing. Some people learn by taking copious notes. Beethoven, for example, left behind an enormous number of sketchbooks, yet he said he never actually looked at them when he composed. Asked why he kept them, he is reported to have replied, “If I don’t write it down immediately, I forget it right away. If I put it into a sketchbook, I never forget it and I never have to look it up again.” Some people learn by doing. Others learn by hearing themselves talk.
Of all the important pieces of self-knowledge, understanding how you learn is the easiest to acquire. When I ask people, “How do you learn?” most of them know the answer. But when I ask, “Do you act on this knowledge?” few answer yes. And yet, acting on this knowledge is the key to performance; or rather, not acting on this knowledge condemns one to nonperformance.
Am I a reader or a listener? and How do I learn? are the first questions to ask. But they are by no means the only ones. To manage yourself effectively, you also have to ask, Do I work well with people, or am I a loner? And if you do work well with people, you then must ask, In what relationship?
Some people work best as subordinates. General George Patton, the great American military hero of World War II, is a prime example. Patton was America’s top troop commander. Yet when he was proposed for an independent command, General George Marshall, the U.S. chief of staff—and probably the most successful picker of men in U.S. history—said, “Patton is the best subordinate the American army has ever produced, but he would be the worst commander.”
Some people work best as team members. Others work best alone. Some are exceptionally talented as coaches and mentors; others are simply incompetent as mentors.
Do not try to change yourself—you are unlikely to succeed. Work to improve the way you perform.
Another crucial question is, Do I produce results as a decision-maker or as an adviser?A great many people perform best as advisers but cannot take the burden and pressure of making the decision. A good many other people, by contrast, need an adviser to force themselves to think; then they can make decisions and act on them with speed, self-confidence, and courage.
This is a reason, by the way, that the number two person in an organization often fails when promoted to the number one position. The top spot requires a decision-maker. Strong decision-makers often put somebody they trust into the number two spot as their adviser—and in that position the person is outstanding. But in the number one spot, the same person fails. He or she knows what the decision should be but cannot accept the responsibility of actually making it.
Other important questions to ask include, Do I perform well under stress, or do I need a highly structured and predictable environment? Do I work best in a big organization or a small one? Few people work well in all kinds of environments. Again and again, I have seen people who were very successful in large organizations flounder miserably when they moved into smaller ones. And the reverse is equally true.
The conclusion bears repeating: Do not try to change yourself—you are unlikely to succeed. But work hard to improve the way you perform. And try not to take on work you cannot perform or will only perform poorly.
What Are My Values?
To be able to manage yourself, you finally have to ask, What are my values? This is not a question of ethics. With respect to ethics, the rules are the same for everybody, and the test is a simple one. I call it the “mirror test.”
In the early years of this century, the most highly respected diplomat of all the great powers was the German ambassador in London. He was clearly destined for great things—to become his country’s foreign minister, at least, if not its federal chancellor. Yet in 1906 he abruptly resigned rather than preside over a dinner given by the diplomatic corps for Edward VII. The king was a notorious womanizer and made it clear what kind of dinner he wanted. The ambassador is reported to have said, “I refuse to see a pimp in the mirror in the morning when I shave.”
That is the mirror test. Ethics requires that you ask yourself, What kind of person do I want to see in the mirror in the morning? What is ethical behavior in one kind of organization or situation is ethical behavior in another. But ethics is only part of a value system—especially of an organization’s value system.
To work in an organization whose value system is unacceptable or incompatible with one’s own condemns a person both to frustration and to nonperformance.
Consider the experience of a highly successful human resources executive whose company was acquired by a bigger organization. After the acquisition, she was promoted to do the kind of work she did best, which included selecting people for important positions. The executive deeply believed that a company should hire people for such positions from the outside only after exhausting all the inside possibilities. But her new company believed in first looking outside “to bring in fresh blood.” There is something to be said for both approaches—in my experience, the proper one is to do some of both. They are, however, fundamentally incompatible—not as policies but as values. They bespeak different views of the relationship between organizations and people; different views of the responsibility of an organization to its people and their development; and different views of a person’s most important contribution to an enterprise. After several years of frustration, the executive quit—at considerable financial loss. Her values and the values of the organization simply were not compatible.
Similarly, whether a pharmaceutical company tries to obtain results by making constant, small improvements or by achieving occasional, highly expensive, and risky “breakthroughs” is not primarily an economic question. The results of either strategy may be pretty much the same. At bottom, there is a conflict between a value system that sees the company’s contribution in terms of helping physicians do better what they already do and a value system that is oriented toward making scientific discoveries.
Whether a business should be run for short-term results or with a focus on the long term is likewise a question of values. Financial analysts believe that businesses can be run for both simultaneously. Successful businesspeople know better. To be sure, every company has to produce short-term results. But in any conflict between short-term results and long-term growth, each company will determine its own priority. This is not primarily a disagreement about economics. It is fundamentally a value conflict regarding the function of a business and the responsibility of management.
Value conflicts are not limited to business organizations. One of the fastest-growing pastoral churches in the United States measures success by the number of new parishioners. Its leadership believes that what matters is how many newcomers join the congregation. The Good Lord will then minister to their spiritual needs or at least to the needs of a sufficient percentage. Another pastoral, evangelical church believes that what matters is people’s spiritual growth. The church eases out newcomers who join but do not enter into its spiritual life.
Again, this is not a matter of numbers. At first glance, it appears that the second church grows more slowly. But it retains a far larger proportion of newcomers than the first one does. Its growth, in other words, is more solid. This is also not a theological problem, or only secondarily so. It is a problem about values. In a public debate, one pastor argued, “Unless you first come to church, you will never find the gate to the Kingdom of Heaven.”
“No,” answered the other. “Until you first look for the gate to the Kingdom of Heaven, you don’t belong in church.”
Organizations, like people, have values. To be effective in an organization, a person’s values must be compatible with the organization’s values. They do not need to be the same, but they must be close enough to coexist. Otherwise, the person will not only be frustrated but also will not produce results.
A person’s strengths and the way that person performs rarely conflict; the two are complementary. But there is sometimes a conflict between a person’s values and his or her strengths. What one does well—even very well and successfully—may not fit with one’s value system. In that case, the work may not appear to be worth devoting one’s life to (or even a substantial portion thereof).
If I may, allow me to interject a personal note. Many years ago, I too had to decide between my values and what I was doing successfully. I was doing very well as a young investment banker in London in the mid-1930s, and the work clearly fit my strengths. Yet I did not see myself making a contribution as an asset manager. People, I realized, were what I valued, and I saw no point in being the richest man in the cemetery. I had no money and no other job prospects. Despite the continuing Depression, I quit—and it was the right thing to do. Values, in other words, are and should be the ultimate test.
Where Do I Belong?
A small number of people know very early where they belong. Mathematicians, musicians, and cooks, for instance, are usually mathematicians, musicians, and cooks by the time they are four or five years old. Physicians usually decide on their careers in their teens, if not earlier. But most people, especially highly gifted people, do not really know where they belong until they are well past their mid-twenties. By that time, however, they should know the answers to the three questions: What are my strengths? How do I perform? and, What are my values? And then they can and should decide where they belong.
Or rather, they should be able to decide where they do not belong. The person who has learned that he or she does not perform well in a big organization should have learned to say no to a position in one. The person who has learned that he or she is not a decision-maker should have learned to say no to a decision-making assignment. A General Patton (who probably never learned this himself) should have learned to say no to an independent command.
Equally important, knowing the answer to these questions enables a person to say to an opportunity, an offer, or an assignment, “Yes, I will do that. But this is the way I should be doing it. This is the way it should be structured. This is the way the relationships should be. These are the kind of results you should expect from me, and in this time frame, because this is who I am.”
Successful careers are not planned. They develop when people are prepared for opportunities because they know their strengths, their method of work, and their values. Knowing where one belongs can transform an ordinary person—hardworking and competent but otherwise mediocre—into an outstanding performer.
What Should I Contribute?
Throughout history, the great majority of people never had to ask the question, What should I contribute? They were told what to contribute, and their tasks were dictated either by the work itself—as it was for the peasant or artisan—or by a master or a mistress—as it was for domestic servants. And until very recently, it was taken for granted that most people were subordinates who did as they were told. Even in the 1950s and 1960s, the new knowledge workers (the so-called organization men) looked to their company’s personnel department to plan their careers.
Then in the late 1960s, no one wanted to be told what to do any longer. Young men and women began to ask, What do I want to do? And what they heard was that the way to contribute was to “do your own thing.” But this solution was as wrong as the organization men’s had been. Very few of the people who believed that doing one’s own thing would lead to contribution, self-fulfillment, and success achieved any of the three.
But still, there is no return to the old answer of doing what you are told or assigned to do. Knowledge workers in particular have to learn to ask a question that has not been asked before: What should my contribution be? To answer it, they must address three distinct elements: What does the situation require? Given my strengths, my way of performing, and my values, how can I make the greatest contribution to what needs to be done? And finally, What results have to be achieved to make a difference?
Consider the experience of a newly appointed hospital administrator. The hospital was big and prestigious, but it had been coasting on its reputation for 30 years. The new administrator decided that his contribution should be to establish a standard of excellence in one important area within two years. He chose to focus on the emergency room, which was big, visible, and sloppy. He decided that every patient who came into the ER had to be seen by a qualified nurse within 60 seconds. Within 12 months, the hospital’s emergency room had become a model for all hospitals in the United States, and within another two years, the whole hospital had been transformed.
As this example suggests, it is rarely possible—or even particularly fruitful—to look too far ahead. A plan can usually cover no more than 18 months and still be reasonably clear and specific. So the question in most cases should be, Where and how can I achieve results that will make a difference within the next year and a half? The answer must balance several things. First, the results should be hard to achieve—they should require “stretching,” to use the current buzzword. But also, they should be within reach. To aim at results that cannot be achieved—or that can be only under the most unlikely circumstances—is not being ambitious; it is being foolish. Second, the results should be meaningful. They should make a difference. Finally, results should be visible and, if at all possible, measurable. From this will come a course of action: what to do, where and how to start, and what goals and deadlines to set.
Responsibility for Relationships
Very few people work by themselves and achieve results by themselves—a few great artists, a few great scientists, a few great athletes. Most people work with others and are effective with other people. That is true whether they are members of an organization or independently employed. Managing yourself requires taking responsibility for relationships. This has two parts.
The first is to accept the fact that other people are as much individuals as you yourself are. They perversely insist on behaving like human beings. This means that they too have their strengths; they too have their ways of getting things done; they too have their values. To be effective, therefore, you have to know the strengths, the performance modes, and the values of your coworkers.
That sounds obvious, but few people pay attention to it. Typical is the person who was trained to write reports in his or her first assignment because that boss was a reader. Even if the next boss is a listener, the person goes on writing reports that, invariably, produce no results. Invariably the boss will think the employee is stupid, incompetent, and lazy, and he or she will fail. But that could have been avoided if the employee had only looked at the new boss and analyzed how this boss performs.
Bosses are neither a title on the organization chart nor a “function.” They are individuals and are entitled to do their work in the way they do it best. It is incumbent on the people who work with them to observe them, to find out how they work, and to adapt themselves to what makes their bosses most effective. This, in fact, is the secret of “managing” the boss.
The same holds true for all your coworkers. Each works his or her way, not your way. And each is entitled to work in his or her way. What matters is whether they perform and what their values are. As for how they perform—each is likely to do it differently. The first secret of effectiveness is to understand the people you work with and depend on so that you can make use of their strengths, their ways of working, and their values. Working relationships are as much based on the people as they are on the work.
The second part of relationship responsibility is taking responsibility for communication. Whenever I, or any other consultant, start to work with an organization, the first thing I hear about are all the personality conflicts. Most of these arise from the fact that people do not know what other people are doing and how they do their work, or what contribution the other people are concentrating on and what results they expect. And the reason they do not know is that they have not asked and therefore have not been told.
This failure to ask reflects human stupidity less than it reflects human history. Until recently, it was unnecessary to tell any of these things to anybody. In the medieval city, everyone in a district plied the same trade. In the countryside, everyone in a valley planted the same crop as soon as the frost was out of the ground. Even those few people who did things that were not “common” worked alone, so they did not have to tell anyone what they were doing.
Today the great majority of people work with others who have different tasks and responsibilities. The marketing vice president may have come out of sales and know everything about sales, but she knows nothing about the things she has never done—pricing, advertising, packaging, and the like. So the people who do these things must make sure that the marketing vice president understands what they are trying to do, why they are trying to do it, how they are going to do it, and what results to expect.
If the marketing vice president does not understand what these high-grade knowledge specialists are doing, it is primarily their fault, not hers. They have not educated her. Conversely, it is the marketing vice president’s responsibility to make sure that all of her coworkers understand how she looks at marketing: what her goals are, how she works, and what she expects of herself and of each one of them.
The first secret of effectiveness is to understand the people you work with so that you can make use of their strengths.
Even people who understand the importance of taking responsibility for relationships often do not communicate sufficiently with their associates. They are afraid of being thought presumptuous or inquisitive or stupid. They are wrong. Whenever someone goes to his or her associates and says, “This is what I am good at. This is how I work. These are my values. This is the contribution I plan to concentrate on and the results I should be expected to deliver,” the response is always, “This is most helpful. But why didn’t you tell me earlier?”
And one gets the same reaction—without exception, in my experience—if one continues by asking, “And what do I need to know about your strengths, how you perform, your values, and your proposed contribution?” In fact, knowledge workers should request this of everyone with whom they work, whether as subordinate, superior, colleague, or team member. And again, whenever this is done, the reaction is always, “Thanks for asking me. But why didn’t you ask me earlier?”
Organizations are no longer built on force but on trust. The existence of trust between people does not necessarily mean that they like one another. It means that they understand one another. Taking responsibility for relationships is therefore an absolute necessity. It is a duty. Whether one is a member of the organization, a consultant to it, a supplier, or a distributor, one owes that responsibility to all one’s coworkers: those whose work one depends on as well as those who depend on one’s own work.
The Second Half of Your Life
When work for most people meant manual labor, there was no need to worry about the second half of your life. You simply kept on doing what you had always done. And if you were lucky enough to survive 40 years of hard work in the mill or on the railroad, you were quite happy to spend the rest of your life doing nothing. Today, however, most work is knowledge work, and knowledge workers are not “finished” after 40 years on the job, they are merely bored.
We hear a great deal of talk about the midlife crisis of the executive. It is mostly boredom. At 45, most executives have reached the peak of their business careers, and they know it. After 20 years of doing very much the same kind of work, they are very good at their jobs. But they are not learning or contributing or deriving challenge and satisfaction from the job. And yet they are still likely to face another 20 if not 25 years of work. That is why managing oneself increasingly leads one to begin a second career.
There are three ways to develop a second career. The first is actually to start one. Often this takes nothing more than moving from one kind of organization to another: the divisional controller in a large corporation, for instance, becomes the controller of a medium-sized hospital. But there are also growing numbers of people who move into different lines of work altogether: the business executive or government official who enters the ministry at 45, for instance; or the midlevel manager who leaves corporate life after 20 years to attend law school and become a small-town attorney.
We will see many more second careers undertaken by people who have achieved modest success in their first jobs. Such people have substantial skills, and they know how to work. They need a community—the house is empty with the children gone—and they need income as well. But above all, they need challenge.
The second way to prepare for the second half of your life is to develop a parallel career. Many people who are very successful in their first careers stay in the work they have been doing, either on a full-time or part-time or consulting basis. But in addition, they create a parallel job, usually in a nonprofit organization, that takes another 10 hours of work a week. They might take over the administration of their church, for instance, or the presidency of the local Girl Scouts council. They might run the battered women’s shelter, work as a children’s librarian for the local public library, sit on the school board, and so on.
Finally, there are the social entrepreneurs. These are usually people who have been very successful in their first careers. They love their work, but it no longer challenges them. In many cases they keep on doing what they have been doing all along but spend less and less of their time on it. They also start another activity, usually a nonprofit. My friend Bob Buford, for example, built a very successful television company that he still runs. But he has also founded and built a successful nonprofit organization that works with Protestant churches, and he is building another to teach social entrepreneurs how to manage their own nonprofit ventures while still running their original businesses.
People who manage the second half of their lives may always be a minority. The majority may “retire on the job” and count the years until their actual retirement. But it is this minority, the men and women who see a long working-life expectancy as an opportunity both for themselves and for society, who will become leaders and models.
There is one prerequisite for managing the second half of your life: You must begin long before you enter it. When it first became clear 30 years ago that working-life expectancies were lengthening very fast, many observers (including myself) believed that retired people would increasingly become volunteers for nonprofit institutions. That has not happened. If one does not begin to volunteer before one is 40 or so, one will not volunteer once past 60.
Similarly, all the social entrepreneurs I know began to work in their chosen second enterprise long before they reached their peak in their original business. Consider the example of a successful lawyer, the legal counsel to a large corporation, who has started a venture to establish model schools in his state. He began to do volunteer legal work for the schools when he was around 35. He was elected to the school board at age 40. At age 50, when he had amassed a fortune, he started his own enterprise to build and to run model schools. He is, however, still working nearly full-time as the lead counsel in the company he helped found as a young lawyer.
There is one prerequisite for managing the second half of your life: You must begin doing so long before you enter it.
There is another reason to develop a second major interest, and to develop it early. No one can expect to live very long without experiencing a serious setback in his or her life or work. There is the competent engineer who is passed over for promotion at age 45. There is the competent college professor who realizes at age 42 that she will never get a professorship at a big university, even though she may be fully qualified for it. There are tragedies in one’s family life: the breakup of one’s marriage or the loss of a child. At such times, a second major interest—not just a hobby—may make all the difference. The engineer, for example, now knows that he has not been very successful in his job. But in his outside activity—as church treasurer, for example—he is a success. One’s family may break up, but in that outside activity there is still a community.
In a society in which success has become so terribly important, having options will become increasingly vital. Historically, there was no such thing as “success.” The overwhelming majority of people did not expect anything but to stay in their “proper station,” as an old English prayer has it. The only mobility was downward mobility.
In a knowledge society, however, we expect everyone to be a success. This is clearly an impossibility. For a great many people, there is at best an absence of failure. Wherever there is success, there has to be failure. And then it is vitally important for the individual, and equally for the individual’s family, to have an area in which he or she can contribute, make a difference, and be somebody. That means finding a second area—whether in a second career, a parallel career, or a social venture—that offers an opportunity for being a leader, for being respected, for being a success.
The challenges of managing oneself may seem obvious, if not elementary. And the answers may seem self-evident to the point of appearing naive. But managing oneself requires new and unprecedented things from the individual, and especially from the knowledge worker. In effect, managing oneself demands that each knowledge worker think and behave like a chief executive officer. Further, the shift from manual workers who do as they are told to knowledge workers who have to manage themselves profoundly challenges social structure. Every existing society, even the most individualistic one, takes two things for granted, if only subconsciously: that organizations outlive workers, and that most people stay put.
But today the opposite is true. Knowledge workers outlive organizations, and they are mobile. The need to manage oneself is therefore creating a revolution in human affairs.
Peter F. Drucker (November 19, 1909 – November 11, 2005) was an Austrian-born American management consultant, educator, and author whose writings contributed to the philosophical and practical foundations of the modern business corporation. He was also a leader in the development of management education, he invented the concept known as management by objectives, and he has been described as “the founder of modern management.”
Eyeing a rivalry with Roche and a new cancer asset slated to hit the markets next year, Bristol Myers Squibb is picking up Turning Point Therapeutics in a $4.1 billion acquisition.
BMS will gain access to repotrectinib, a midstage candidate in testing for first-line lung cancer as a potential competitor to Roche’s Rozlytrek. The Big Pharma landed Turning Point for $76 per share, with both companies’ boards approving the transaction that is slated to close in the third quarter.
The buy will bolster BMS’s medium- to long-term growth strategy, providing a pipeline of precision oncology medicines that target common mutations that cause the growth of cancer cells. The star is of course the lead asset repotrectinib, a next-generation tyrosine kinase inhibitor that targets the ROS1 and NTRK gene mutations—just like Rozlytrek.
The Roche med, which was approved in 2019, brought in 16 million Swiss francs ($16.6 million) for the Swiss pharma in the first quarter, a 78% increase over the same quarter a year before. The therapy is approved in a type of mutated non-small cell lung cancer (NSCLC), solid tumors and ROS1-positive, advanced non-small cell lung cancer.
Repotrectinib has earned three breakthrough-therapy tags and has demonstrated a longer duration of response compared to existing ROS1 agents in first-line NSCLC during a phase 1/2 trial. Other studies involving the med include late-stage adult and pediatric advanced solid tumor trials and an earlier stage KRAS-targeting combination study.
The therapy is expected to be approved in the U.S. in the second half of 2023, according to BMS. The Big Pharma will also “explore the potential” of Turning Point’s other candidates, which include the solid tumor therapies elzovantinib and TPX-0046.
Turning Point President and CEO Athena Countouriotis, M.D., said with BMS’ commercial capabilities and manufacturing footprint, the biotech can accelerate efforts to bring its medicines to patients. BMS CEO Giovanni Caforio, M.D., meanwhile, said the acquisition continues the company’s “strong track record of strategic business development to further enhance our growth profile.”
SVB Securities analysts said the deal represents a 122% premium from Turning Point’s previous close of $34.16. But the shares skyrocketed upward Friday afternoon on the news of the deal to $74 apiece—a 116% increase and a gain of nearly $40. This reflects SVB Securities’ expectation of “little resistance from investors” given the tough biotech markets and the fact that many companies are trading at or below cash.
The firm predicts the market potential for repotrectinib to be $1.14 billion in the first-line setting and $455 million in the second line at peak. But this may take a few quarters after launch, into 2024, to realize. Turning Point is expected to meet with the FDA soon to discuss the filing, which could occur by the end of the year.
During that meeting, Turning Point is expected to get clarity on whether an accelerated approval might be an option for repotrectinib and whether the therapy could be submitted for a “line agnostic” ROS-1 indication, meaning it could be used at whatever stage of treatment for patients with the matching gene mutation. The company will also learn whether any confirmatory or post-approval studies will be needed, which is the case when an accelerated approval is granted.
“While we are not privy to the specifics of the deal or [Bristol’s] expectations for this meeting, we think it is unlikely to derail the deal given that the drug has three breakthrough therapy designations, suggesting that the agency views the compound as significantly differentiated,” SVB Securities wrote.
BMS has several therapies approved or in development for NSCLC, including Opdivo, Yervoy, Opdualag and CC-90011; however, SVB Securities does not believe this will raise any antitrust red flags given none of those target ROS1.
Repotrectinib (ROS1/NTRK Inhibitor)는 2023년말에 FDA 승인을 받아서 Augtyro라는 브랜드명으로 판매되고 있습니다. 이로써 Turning Point Therapeutics 팀의 실력이 입증된 셈입니다.
On November 15, 2023, the Food and Drug Administration approved repotrectinib (Augtyro, Bristol-Myers Squibb Company) for locally advanced or metastatic ROS1-positive non-small cell lung cancer (NSCLC).
This is the first FDA approval that includes patients with ROS1-positive NSCLC who have previously received a ROS1 tyrosine kinase inhibitor (TKI), in addition to patients who are TKI naïve.
The full prescribing information for Augtyro will be posted here.
Approval was based on TRIDENT-1, a global, multicenter, single-arm, open-label, multi-cohort clinical trial (NCT03093116) which included patients with ROS1-positive locally advanced or metastatic NSCLC. Efficacy was evaluated in 71 ROS1 TKI-naïve patients who received up to 1 prior line of platinum-based chemotherapy and/or immunotherapy and 56 patients who received 1 prior ROS1 TKI with no prior platinum-based chemotherapy or immunotherapy.
The major efficacy outcome measures were overall response rate (ORR) and duration of response (DOR) according to RECIST v1.1 as assessed by blinded independent central review. Confirmed ORR in the ROS1 TKI naïve group was 79% (95% CI: 68, 88) and 38% (95% CI: 25, 52) in those patients receiving prior treatment with a ROS1 inhibitor. Median DOR was 34.1 months (95% CI: 25.6, not evaluable) and 14.8 months (95% CI: 7.6, not evaluable) in the two respective groups. Responses were observed in intracranial lesions in patients with measurable CNS metastases, and in patients with resistance mutations following TKI therapy.
The most common (>20%) adverse reactions were dizziness, dysgeusia, peripheral neuropathy, constipation, dyspnea, ataxia, fatigue, cognitive disorders, and muscular weakness.
The recommended repotrectinib dose is 160 mg orally once daily with or without food for 14 days, then increased to 160 mg twice daily, until disease progression or unacceptable toxicity.
This review used the Assessment Aid, a voluntary submission from the applicant to facilitate the FDA’s assessment.
Repotrectinib (ROS1/NTRK Inhibitor)의 FDA 승인이 있기 전에 Turning Point의 CEO와 CMO였던 Athena Countouriotis 박사와 Mohammad Hirmand 박사는 Avenzo Therapeutics를 설립하고 Orbimed, SR One, Lilly Asia Ventures 등 굵직한 VC의 펀딩으로 $200 Million Seed & Series A round를 마칩니다. Avenzo의 비즈니스 모델은 초기 oncology small molecules, ADCs 등을 확보하는 것이고 중국 바이오텍으로 부터 중국 이외의 권리를 인수해서 속히 나스닥에 상장하고 약물을 성공시킨다는 전략입니다.
The crew at Turning Point Therapeutics is back together for a new biotech that wants to acquire early-stage oncology small molecules, including antibody drug conjugates, and potentially form partnerships with China-based drug developers for ex-China rights as it eyes a speedy leap onto the Nasdaq around this time next year, CEO Athena Countouriotis told Endpoints News.
After selling Turning Point to Bristol Myers Squibb, announced at the onset of last year’s ASCO confab, she and colleague Mohammad Hirmand founded Avenzo Therapeutics. The CEO and CMO already have approximately $200 million in seed and Series A financing from five big-name investors to evaluate which drugs to bring into its pipeline. That includes SR One, OrbiMed, Foresite Capital, Citadel’s Surveyor Capital and Lilly Asia Ventures. Bidding wars for assets have led Avenzo to miss out on some deals in recent months, but the biotech has three active term sheets and hopes to bring in its first asset in the third quarter, Countouriotis said in a Friday morning interview.
Following that deal, Avenzo will likely look to raise a Series B of similar size before going onto the Nasdaq, for which the startup already has a ticker symbol in mind, the CEO said. She has invested in the company herself and named it after her two children, Ava and Enzo.
Conversations are already underway with companies that no longer have clinical plans for certain therapeutic candidates or are cash-constrained, Countouriotis told Nasdaq in a recent interview. With the help of Lilly Asia Ventures, Avenzo will also scour ADC opportunities in China, where recent deals have come together for Duality Biologics with BioNTech and MediLink Therapeutics with Zai Lab. The one area Avenzo is shying away from is cell and gene therapy, the CEO said, noting the manufacturing spending required.
Avenzo’s story seems rare today, but has the hallmarks of 2020-2021 biotech ambitions: quick financing, blue-chip VC firms coming together to back executives with IPO and M&A chops, assets that haven’t been through much clinical testing and a speedy flip onto the public markets.
Avenzo’s path also sounds familiar to Acelyrin’s: raise massive private rounds to bankroll the licensing of other companies’ drugs and then take them through the clinic. Earlier this month, Acelyrin, led by former Horizon Therapeutics executives, went public in one of biopharma’s largest IPOs in years.
Speaking with Nasdaq, Countouriotis said San Diego-based Avenzo is still in “stealth mode,” a term used endlessly in biotech circles. With eight employees in Avenzo’s infancy, the CEO hopes to grow the company like she did at Turning Point, which went public in 2019 and then sold for $4.1 billion last summer, growing from less than 20 employees to 300-plus during her tenure.
전략대로 중국의 Allorion Therapeutics로 부터 임상1상에 있는 CDK2 blocker AVZO-021을 $40 Million upfront & $1 Billion total 가격으로 인수합니다.
Avenzo Therapeutics, Merck KGaA and AbbVie each inked new deals to top up their cancer pipelines, with the former two companies handing over a combined $85 million in upfront cash.
Avenzo disclosed Thursday that it has locked arms with Allorion Therapeutics, snapping up ex-Greater China rights to the early-stage CDK2 blocker AVZO-021. The enzyme has been shown to hamper the impact of CDK4 or CDK6-targeting therapies in patients with HR-positive/HER2-negative breast cancer and can drive tumor development in other kinds of cancers, according to Avenzo. The med is currently in a phase 1 trial in patients with breast cancer and other patients with solid tumors. Avenzo can also tack on a preclinical asset from Allorion slated for IND submission in early 2025.
In exchange, Avenzo is paying Allurion $40 million upfront with more than $1 billion in biobucks attached to milestones for both AVZO-021 and the preclinical program. The money comes from nearly $200 million in funds raised in the middle of 2023, thanks to the likes of Lilly Asia Ventures and SR One.
Avenzo is the latest venture from ex-Turning Point CEO Athena Countouriotis, M.D., who helped lead a $4.1 billion buyout from Bristol Myers Squibb in June 2022.
Avenzo wasn’t the only biotech to hit the dealmaking trail, with Merck KGaA tacking on ex-US licensing rights to Inspirna’s phase 2 colorectal cancer med, ompenaclid. Inspirna has aimed the med specifically at patients with RAS-mutated, advanced forms of the cancer, showing at last year’s European Society for Medical Oncology annual meeting that the drug produced a 37% objective response rate in 30 evaluable patients. The median progression-free survival was 10.2 months in a slightly larger sample size of 41 patients.
The German pharma is paying $45 million upfront with an undisclosed amount of biobucks on the table. Merck also has the option to co-develop and co-commercialize the med in the U.S. alongside Inspirna.
Last but certainly not least, AbbVie, fresh off its end-of-the-year shopping spree, is heading back to the deal well, this time for Umoja’s cell therapies. The top prize is licensing rights to Umoja’s lead in-situ candidate UB-VV111, currently in IND-enabling studies. The asset is the first test of Umoja’s in-vivo CAR-T, aiming to break some of the limitations associated with current autologous manufacturing processes. Umoja plans to ask regulators to enter a phase 1 trial in the first half of this year.
The second part of the deal is a larger discovery pact for up to four additional in-situ candidates, aimed at targets selected by AbbVie. All told, Umoja received both an undisclosed upfront payment and equity investment, with $1.4 billion in milestone payments available.
AVZO-021을 인수하고 2달이 지나서 $150 Million Series A-1을 받았습니다. 이번에는 Sofinnova가 들어왔습니다. AVZO-021은 기존 CDK4/6 inhibitor에 저항성을 가진 환자들을 대상으로 한다는 전략입니다.
San Diego-based Avenzo Therapeutics on Tuesday announced that it has closed a $150 million oversubscribed Series A-1 funding round, which the biotech will use to develop novel oncology therapeutics.
Tuesday’s haul brings Avenzo’s total capital raised to $347 million since it was founded in August 2022, according to the company. The Series A-1 was led by New Enterprise Associates, Deep Track Capital, Sofinnova Investments and Sands Capital. New backers include Quan Capita, Delos Capital and TF Capital.
Avenzo CEO Athena Countouriotis in a statement said that the company has “made great progress” in its aim to “advance the next generation of oncology therapies for patients,” including its lead program AVZ-021, a potentially best-in-class CDK2 selective inhibitor.
According to Avenzo’s website, most FDA-approved inhibitors target the CDK4/6 axis, which in turn helps prevent the abnormal cell proliferation central to cancers. However, most patients develop resistance to CDK4/6 inhibitors through the hyperactivation of the CDK2 pathway. AVZ-021 works by blocking this cascade, which when used with CDK4/6 inhibitors could overcome such resistances and induce durable treatment responses.
AVZ-021 was originally developed by the Boston- and China-based Allorion Therapeutics, which demonstrated in pre-clinical studies that the candidate selectively targeted CDK2 over CDK1, which is otherwise a driver of treatment toxicity. In January 2024, Avenzo paid $40 million upfront in an exclusive licensing deal with Allorion, which also includes an option for an additional preclinical program.
Avenzo also pledged more than $1 billion in development, regulatory and commercial milestones, plus tiered royalties, for both programs.
In collaboration with Allorion, Avenzo is running a Phase I/II study to evaluate AVZ-021 in patients with HR+/HER2- metastatic breast cancer and other advanced solid tumors.
The first part of the study is a dose-escalation phase to evaluate the safety and tolerability of the candidate, as well as determine a recommended Phase II dose. The partners will then test AVZ-021 in a Phase II dose-expansion study to evaluate the antitumor activity of the candidate. The trial is currently recruiting in the U.S.
“We are in a strong position to advance our potentially best-in-class CDK2 inhibitor, AVZO-021, expand our pipeline with additional assets, and continue to grow our team,” Countouriotis said.
With its oversubscribed Series-A1, Avenzo follows in the footsteps of other San Diego biotechs that have recently reported sizable funding hauls. Last week, Capstan Therapeutics announced that it had closed a $175 million Series B funding round to develop its in vivo CAR-T cell therapy candidate. Mirador Therapeutics also launched last week, securing $400 million in funds to advance inflammatory and fibrotic disease programs.
설립한지 이제 1년이 채 되지 않았기 때문에 파이프라인은 한개입니다. 계속 초기 약물을 사서 파이프라인을 붙여나갈 것으로 기대합니다.
(Picture: Marcis Souza, CEO of Praxis Precision Medicines)
안녕하세요 보스턴 임박사입니다.
미국 바이오텍 기업들이 나스닥 상장 이전에는 펀딩 이력을 꼭 정확히 공표하지 않는 경우도 있습니다. 회사의 경쟁력을 확보하기 위해서 Stealth Mode로 오랜기간 있는 경우가 있죠.
Praxis Precision Medicines는 Private Equity Firm인 Blackston Life Sciences의 펀딩으로 오랜기간 파이프라인 준비를 하고 2020년이 되어서야 $100 Million 펀딩 소식을 발표했습니다. 이 펀딩은 시리즈 B인 것으로 보입니다. 파이프라인 중 가장 앞선 것은 allosteric GABAA modulator인 PRAX-114였고 Calcium channel blocker인 Ulixacaltamide (PRAX-944)가 뒤를 따르고 있다고 발표했습니다.
Praxis Precision Medicines is coming out of the shadows with $100 million from the likes of Blackstone Life Sciences and a pipeline of central nervous system (CNS) programs. The cash will bankroll a pivotal study for a depression drug as well as push earlier stage programs into the clinic.
As suggested by its name, Praxis aims to do for brain disorders what precision medicine has done for cancer treatment. Its pipeline targets genes that control the imbalance in neuronal signaling that underlies CNS disorders, both prevalent and rare. Since its inception, the Cambridge, Massachusetts-based biotech has banked $100 million from the likes of Novo Holdings, Vida Ventures and Eventide.
Praxis has two candidates in phase 2: PRAX-114, a positive allosteric modulator of GABAA receptors in development for major depressive disorder and perimenopausal depression, and PRAX-944, which blocks a type of calcium channel to treat essential tremor.
“As was achieved in oncology decades ago, recent genetic insights have presented meaningful opportunities to treat brain disorders in entirely different and targeted ways based on the specific genetically validated pathways driving a patient’s disease,” said Kiran Reddy, M.D., a venture partner at Blackstone Life Sciences, Praxis’ founding investor. “We are reducing these insights to practice, to create novel medicines that could fundamentally alter the treatment path and outcomes for patients with brain disorders.”
Reddy’s fellow founders include Chief Scientific Officer Steven Petrou, Ph.D., director of the Florey Institute of Neuroscience and Mental Health at the University of Melbourne in Australia, and David Goldstein, Ph.D., who leads the Institute for Genomic Medicine at Columbia University.
At the helm is Marcio Souza, who joined from PTC Therapeutics, where he has worn several hats since 2014, most recently serving as its chief operating officer.
Over the next year, Praxis plans to start a pivotal study of PRAX-114 in major depressive disorder and release proof-of-concept data for PRAX-944 in essential tremor. It also aims to push its earlier-stage programs into the clinic, including treatments for rare epilepsies.
Praxis Precision Medicines, a clinical-stage, genetic neuroscience company, launched today with more than $100 million in financing since its inception from premier life science investors led by founding investor Blackstone Life Sciences (via prior Clarus funds in 2016) as well as Novo Holdings, Vida Ventures, Eventide and other prominent funds. Praxis is deploying a precision medicine approach to develop high-impact therapies that target the underlying causal mechanisms of both prevalent and rare brain disorders with overlapping disease biology.
“Neurology and psychiatry are finally primed for a revolution in how new therapies are discovered and developed, and Praxis’ approach has the potential to change the treatment landscape,” said Marcio Souza, president and chief executive officer of Praxis. “The combination of the expertise of our team in CNS drug development, insights into CNS biology, and our approach to drug discovery, positions us as at the forefront of the development of novel CNS therapies.”
“Depression, and more broadly, psychiatric and neurological disorders are a large and increasing unmet medical need with profound implications on the economy. Praxis aims to leverage the recent breakthroughs in genetics to develop innovative medicines that can improve the lives of the many patients who need them,” said Nicholas Galakatos, Ph.D., chairman of the Praxis board of directors and global head of Blackstone Life Sciences.
Praxis Approach and Pipeline
Praxis is leveraging recent discoveries in the genetics of epilepsy, which have elucidated genes, that when dysregulated, drive a range of neuropsychiatric and movement disorders. Using these insights, Praxis is rapidly advancing a pipeline of treatments that specifically address genes controlling the imbalance of excitation and inhibition of neuronal circuitry at the core of multiple CNS disorders. The company’s portfolio is led by PRAX-114, a GABAA positive allosteric modulator (PAM) in Phase 2 development for the treatment of major depressive disorder (MDD) and perimenopausal depression, and PRAX-944, a T-type calcium channel blocker, in Phase 2 development for the treatment of essential tremor. Within the next year, Praxis plans to initiate its first pivotal trial for PRAX-114 in MDD, report proof-of-concept data for PRAX-944 in essential tremor and advance its earlier stage programs into clinical development for rare epilepsies and other neurological disorders with genetically validated mechanisms.
“As was achieved in oncology decades ago, recent genetic insights have presented meaningful opportunities to treat brain disorders in entirely different and targeted ways based on the specific genetically validated pathways driving a patient’s disease,” said Kiran Reddy, M.D., co-founder and member of Praxis’ board of directors. “We are reducing these insights to practice, to create novel medicines that could fundamentally alter the treatment path and outcomes for patients with brain disorders.”
Internationally Recognized Founding Team
Praxis’ founders are renowned scientists and clinicians leading the industry’s growing understanding of the genetics and biology of disease-causing targets in psychiatric and neurologic disorders.
Dr. Reddy is a venture partner and senior advisor at Blackstone Life Sciences. He was previously on the corporate strategy leadership team at Biogen and was an associate partner at Third Rock Ventures, where he co-founded multiple biotech companies. Dr. Reddy is a neurologist and started his career in academic medicine at Harvard/Massachusetts General Hospital.
Co-founder David Goldstein, Ph.D. is the Director of The Institute for Genomic Medicine, and Professor in the Department of Genetics and Development, at Columbia University. Dr. Goldstein’s work focuses on broad aspects of precision medicine and is widely recognized for multiple influential studies in population and human genetics, including those of the Epi4K consortium that discovered and characterized novel epilepsy genes.
Co-founder and chief scientific officer, Steven Petrou, Ph.D. is the Director of the Florey Institute of Neuroscience and Mental Health, Head of the Department of the Florey Institute at the University of Melbourne in Australia, heads the Ion Channels and Human Disease Laboratory. Prof. Petrou is a recognized leader in the field of ion channel neuropathies in rare pediatric epilepsies and other neurodevelopmental disorders. His published interdisciplinary research has focused on functional genetics and genomics of epilepsy, elucidation of mechanisms of disease, development of several of the first animal models of genetic epilepsy and discovery and evaluation of consequent precision medicine approaches.
Successful Biotech CEO and Leadership Team
Prior to joining Praxis as president and chief executive officer, Mr. Souza was at PTC Therapeutics, where he served in leadership roles since 2014, most recently serving as chief operating officer. He also served in leadership roles in the U.S. and globally at NPS Pharmaceuticals, Shire and Genzyme. Mr. Souza holds a degree in pharmacy and biochemistry from University of São Paulo and an MBA from Fundação Dom Cabral in Brazil.
The Praxis leadership team is comprised of recognized leaders in neuroscience drug discovery, development, and commercialization, including Bernard Ravina, M.D., M.S., chief medical officer; Stuart Chaffee, Ph.D., MBA, chief business officer; Dr. Petrou., co-founder and chief scientific officer; Marion Wittmann, Ph.D., vice president of biology; Gabriel Martinez, Ph.D., vice president of chemistry; Rosa Tarng, vice president, portfolio management; and Karl Hansen, Ph.D., senior vice president, CMC.
About Praxis Precision Medicines
Praxis Precision Medicines is a clinical-stage genetic neuroscience company developing breakthrough therapies for patients and families affected by complex and debilitating brain disorders, including psychiatric disorders, movement disorders and rare pediatric epilepsies. These disease areas share overlapping genetics and neurocircuit biology, as well as a profound need for new therapeutic options that target the underlying cause of the disease. Praxis is advancing a pipeline of breakthrough medicines with the potential to more precisely treat brain disorders. For more information, please visit www.praxismedicines.com.
시리즈 B를 발표한지 2달만에 시리즈 C-1 $110 Million을 발표했습니다. 앞의 두개 파이프라인에 간질 및 통증 치료제인 PRAX-562가 추가된 것으로 공개했습니다.
Praxis Precision Medicines has raised $110 million to take its three clinical-phase central nervous system treatments forward. The pipeline is led by a GABAA positive allosteric modulator that is closing in on the start of a pivotal trial in depression.
Praxis kept a low profile in its early years, only breaking cover to disclose financings in Securities and Exchange Commission filings and publish the starts of clinical trials on registry platforms. The secretive approach was made possible by the support of deep-pocketed founding backer Blackstone Life Sciences, nee Clarus.
By the time Praxis uncloaked in May, the biotech had raised more than $100 million and moved to within one year of the start of a pivotal trial of its lead asset. That candidate, PRAX-114, was trailed closely by another phase 2 asset, PRAX-944, and a then-undisclosed prospect that has now joined the two more advanced prospects in the clinic.
With three clinical programs underway and a pivotal trial on the horizon, Praxis has pulled in more money to fund its R&D activities. Eventide Asset Management led the series C1 round with support from fellow existing investors Vida Ventures, Novo Holdings, Blackstone Life Sciences and OCV Partners. Praxis also disclosed investment from nine first-time backers including Avoro Capital Advisors and Qatar Investment Authority.
The $110 million round will support development of PRAX-114, which is in phase 2 development in major depressive disorder (MDD) and perimenopausal depression. Praxis is testing oral formulations of the GABAA positive allosteric modulator, making its approach similar to Sage Therapeutics’ stuttering effort to bring SAGE-217 to market. SAGE-217 failed a phase 3 trial last year, leading Sage to propose starting three new trials in postpartum depression and subsets of MDD patients.
Praxis’ second clinical candidate, PRAX-944, is a T-type calcium channel blocker in development as a treatment for essential tremor. That therapeutic idea has attracted other companies. Last year, Jazz Pharmaceuticals bought Cavion for T-type calcium channel modulator CX-8998. In May, Neurocrine Biosciences took up its option on Idorsia’s T-type calcium channel blocker ACT-709478.
The two lead assets are trailed by PRAX-562, a phase 1 treatment for genetic epilepsies and pain, and another two treatments for genetic epilepsies that are yet to reach the clinic. The indications targeted by the pipeline reflect Praxis’ belief that it can use new understanding about the genetic causes of epilepsy to develop treatments for diseases driven by the same brain circuits.
그리고 3개월 후에 Nasdaq IPO를 했습니다. 가격과 주식수가 늘어서 결국 $190 Million이나 되는 큰 규모를 할 수 있었습니다. 전광석화같이 보이지만 2020년 이전의 활동이 비공개여서 그 준비기간이 매우 잘 되었다고 생각할 수 있습니다.
2020 is turning out to be a big year for Praxis Precision Medicines. After launching in May with $100 million, the CNS-focused biotech wasted no time topping up its coffers with another $110 million. Now, it’s pulled off a $190 million IPO, upgrading from the $100 million listing it originally sought in September and the revised goal of $175 it set on Thursday.
The old plan was to sell 7.4 million shares at a price between $16 and $18 apiece, but the company bumped the offering up to 10 million shares at $17 to $18 each. Praxis ended up selling the 10 million shares at $19 apiece.
As its name suggests, Praxis is taking aim at the genetic underpinnings of brain disorders to create precision medicines for them. It has three programs in the clinic for depression, essential tremor, epilepsy and pain.
About $70 million to $80 million of the IPO proceeds will bankroll the phase 2a and phase 2/3 trials of lead asset PRAX-114, an oral modulator of GABAA receptors, according to a securities filing. The company is testing the drug in major depressive disorder and perimenopausal depression.
The company tagged $30 million to $40 million to see a second program, PRAX-944, through phase 2a and phase 2/3 studies in essential tremor. Another $20 million to $30 million will fund a phase 1 study in healthy people, as well as the first patient trial, for PRAX-562, a treatment for genetic epilepsies and pain disorders.
All told, the IPO proceeds, along with its previous funding rounds, should carry Praxis through the next 18 months, the company said in the filing.
IPO한지 1년 후 $91 Million 주식공모를 해서 현금을 늘렸습니다. 파이프라인은 여전히 PRAX-114, Ulixacaltamide (PRAX-944) 및 PRAX-562로 세개 프로그램이 진행 중이었습니다.
Praxis Precision Medicines, Inc. (NASDAQ: PRAX), a clinical-stage biopharmaceutical company translating genetic insights into the development of therapies for central nervous system disorders (CNS) characterized by neuronal imbalance, today announced that it has priced an underwritten public offering of 5,000,000 shares of its common stock at a public offering price of $18.25 per share. The gross proceeds to Praxis from the offering are expected to be approximately $91.25 million, before deducting the underwriting discounts and commissions and other offering expenses. Praxis has granted the underwriters a 30-day option to purchase up to an additional 750,000 shares of its common stock.
All shares in the offering are to be sold by Praxis. The offering is expected to close on or about May 18, 2021, subject to satisfaction of customary closing conditions. Praxis intends to use the net proceeds from the offering, together with its existing cash, cash equivalents and short-term investments, to (i) advance PRAX-114 into and through the completion of the Phase 2/3 Aria Study in monotherapy major depressive disorder (“MDD”), which is intended to satisfy one of two registrational trials required by the U.S. Food and Drug Administration to support clinical efficacy for monotherapy MDD, advance PRAX-114 into and through the completion of Praxis’ Phase 2 trial for the adjunctive treatment of MDD, complete Part B (perimenopausal depression) of the Phase 2a clinical trial for PRAX-114, initiate a Phase 3 monotherapy trial in MDD, initiate and complete a Phase 2 trial in post-traumatic stress disorder (“PTSD”), initiate and complete a Phase 2 trial in essential tremor (“ET”) and pursue the development of PRAX-114 in an additional indication; (ii) complete its ongoing Phase 2a clinical trial and a Phase 2 randomized, controlled clinical trial for PRAX-944 in ET and initiate and complete a Phase 2 trial of PRAX-944 in Parkinson’s Disease; (iii) complete its ongoing PRAX-562 Phase 1 healthy volunteer trial and initiate and complete Phase 2 trials of PRAX-562 in Short-lasting Unilateral Neuralgiform headache attacks with Conjunctival injection and Tearing (“SUNCT”), Short-lasting Unilateral Neuralgiform headache with Autonomic symptoms (“SUNA”), and Trigeminal Neuralgia (“TN”), and in developmental and epileptic encephalopathies (“DEEs”), including SCN8A-DEE and SCN2A-DEE, and (iv) advance other programs in its pipeline and support working capital and other general corporate purposes.
BofA Securities, Cowen and Piper Sandler are acting as joint bookrunning managers for the offering, and Wedbush PacGrow is acting as lead manager for the offering.
2022년 1월에 Epilepsia 논문에 PRAX-562의 전임상 연구결과를 발표하였습니다. 기존에 승인된 NaV blockers에 비해 월등히 우수한 약효 를 확인했습니다.
Sage의 Zuranolone에 대항하는 Praxis의 약물 PRAX-114는 primary end points, secondary end points 모두 실망스러운결과를 얻었습니다. 이로 인해 정리해고와 함께 PRAX-562와 PRAX-944 프로그램에 집중하는 것으로 전략이 신속히 수정되었습니다. 가장 선도하던 약물이 실패했을 때, 어떻게 회사를 Turnaround해야 하는지에 대해 잘 보여주는 사례입니다.
Praxis Precision Medicines’ challenge to Sage Therapeutics has unraveled. With a phase 2/3 clinical trial in major depressive disorder (MDD) failing comprehensively, Praxis is stopping work on a clutch of other studies, laying off staff and pinning its hopes on two other candidates.
The failed candidate, PRAX-114, is a type of nervous system drug known as an extrasynaptic GABAA receptor preferring positive allosteric modulator. Sage has gone some way toward validating the mechanism of action with its own drug zuranolone. Yet, Praxis’ bid to improve on the competition by providing a fast, durable antidepressant effect across MDD symptoms, a wider therapeutic window and simple nightly dosing has come unstuck.
Praxis is yet to share data from the phase 2/3 Aria trial, but everything that is known is bad. The study failed its primary endpoint, which looked at change in a depression score at Day 15, and missed all of its secondary endpoints.
“We are surprised and disappointed in the Aria study results,” Praxis CEO Marcio Souza said in a June 6 statement. “PRAX-114 was well-tolerated … yet the effect did not deliver to meet the needs of patients. Praxis is committed to our mission to help people suffering from CNS disorders and will prioritize our programs in movement disorders and epilepsy moving forward.”
The prioritization of the movement disorder and epilepsy programs will see Praxis lay off staff—it had 139 employees as of mid-February, up from 62 at the end of 2020—and stop work on other PRAX-114 trials. The biotech is also closing screening in its phase 2 Acapella study in MDD, positioning it to deliver results in the third quarter, stopping enrollment in a post-traumatic stress disorder phase 2 trial and discontinuing an essential tremor trial.
Through the changes, Praxis expects to extend its cash runway into 2024, giving it the time to rebuild its pipeline around its drugs PRAX-944 and PRAX-562. Top-line results from a phase 2b clinical trial of T-type calcium channel blocker PRAX-944 in the daytime treatment of essential tremor are due in the second half of the year, the same period given for epilepsy prospect PRAX-562 to enter phase 2 trials.
Praxis needs positive data on the candidates to drum up renewed enthusiasm for its pipeline. Shares in the biotech fell more than 60% to around $3 in premarket trading following news of the phase 2/3 flop.
위기는 기회를 동반한다고 하죠. PRAX-114의 실패, 정리해고와 PRAX-562의 Clinical Hold 후 다시 임상 재개 등 어려운 1년을 보낸데 대한 보상과 같은 UCB와 최대 $100 Million 규모의 공동연구계약을 맺습니다. KCNT-1 related epilepsy 프로그램으로 라이선싱 옵션이 있는 딜이었습니다.
It’s been a tough year of layoffs and pipeline culls for Praxis Precision Medicines, but the biotech is ending 2022 on a positive note courtesy of a collaboration with UCB to develop a potential first-ever treatment for a specific type of epilepsy.
The collaboration is based upon Praxis’ PRAX-020 program to discover small-molecule therapeutics as potential treatments of KCNT1-related epilepsies, for which there are currently no approved treatments. As well as an upfront payment from the Belgian biopharma, Praxis will be eligible for development and commercial milestone payments to the tune of up to $100 million, on top of royalties. UCB retains an exclusive option to in-license global development and commercialization rights to any KCNT1 small-molecule candidate that results from the agreement.
The money will come as welcome news to Praxis, which laid off staff and halted a clutch of clinical trials after its nervous system drug PRAX-114 failed to deliver in a phase 2 study in June. The company moved to prioritize its programs in movement disorders and epilepsy, a decision that appears to have paid off with the UCB deal.
Not that Praxis’ bank account is empty—the Boston-based company had $123.7 million in cash and equivalents as of the end September. It may be a drop of over $150 million on the funds the biotech entered the year with, but Praxis reckoned it was still enough to fund it through the start of 2024, even before any payments from UCB are taken into account.
“Our internal research efforts give us confidence that small molecules can selectively inhibit the KCNT1 channel and potentially could be an effective treatment for individuals suffering from KCNT1-related epilepsy,” Praxis CEO Marcio Souza said in a postmarket release Tuesday. “The collaboration with UCB validates this approach and will allow us to accelerate efforts toward a potential treatment for KCNT1 patients.”
As well as a number of other potential epilepsy programs in preclinical development, Praxis has one already in phase 2, with others due to enter phase 1 and 2 before the end of the year. One of these, PRA-562, was recently released from an FDA clinical hold.
Praxis의 Lead Program인 Ulixacaltamide (PRAX-944)의 임상3상 진입과 함께 $63 Million Public financing을 할 수 있었습니다.
Praxis Precision Medicines, Inc. (NASDAQ: PRAX), a clinical-stage biopharmaceutical company translating genetic insights into the development of therapies for central nervous system (CNS) disorders characterized by neuronal excitation-inhibition imbalance, today announced the closing of the underwritten public offering of shares of common stock and pre-funded warrants, including the full exercise of the underwriters’ overallotment option. The net proceeds from the offering are $63.3 million, after deducting underwriting discounts and commissions and estimated offering expenses. Together with the Company’s existing cash, cash equivalents and marketable securities, this extends the cash runway into the first quarter of 2025. The proceeds will be used to advance the development of ulixacaltamide into two Phase 3 studies for essential tremor, to continue clinical development of PRAX-562, PRAX-222 and PRAX-628 for various epilepsies, and for working capital and other general corporate purposes.
The Company has initiated a study evaluating PRAX-628 in photo-sensitive epilepsy patients, also known as a PPR study, with expected readout by year end. Similar studies have shown a positive correlation to anti-seizure medicines (ASMs) used to treat focal epilepsy. With this study, Praxis plans to validate the mechanism of action of PRAX-628 and inform the study design for its Phase 2b program.
Praxis remains on-track for reading out the Phase 2 Study for PRAX-562 and the first cohort for PRAX-222 in DEEs by year end.
“This financing provides the means to continue advancing our portfolio in movement disorders and in epilepsy closer to patients, with a number of catalysts this year,” said Marcio Souza, president and chief executive officer of Praxis. “We are excited to advance our Phase 3 program in essential tremor, while also initiating the PPR study to inform and de-risk our program in focal epilepsy. Additionally, we are pleased to have received support from both existing and new investors.”
About Praxis Praxis Precision Medicines is a clinical-stage biopharmaceutical company translating insights from genetic epilepsies into the development of therapies for CNS disorders characterized by neuronal excitation-inhibition imbalance. Praxis is applying genetic insights to the discovery and development of therapies for rare and more prevalent neurological disorders through our proprietary small molecule platform, Cerebrum™, and antisense oligonucleotide (ASO) platform, Solidus™, using our understanding of shared biological targets and circuits in the brain. Praxis has established a diversified, multimodal CNS portfolio including multiple programs across movement disorders and epilepsy, with four clinical-stage product candidates. For more information, please visit www.praxismedicines.com and follow us on Facebook, LinkedIn and Twitter.
2023년 8월에 ulixacaltamide (PRAX-944)의 임상2상 결과를 발표했고 결과는 좋았습니다. 이 결과는 MDD International Conference에서 발표했습니다.
2024년 3월에 발표한 Corporate Presentation에 의하면 현재 파이프라인은 아래와 같습니다. Small Molecule Platform과 Antisense Oligonucleotide Platform으로 나뉘어져 있고 Ulixacaltamide (PRAX-944)가 임상3상으로 올해 하반기에 Pivotal result가 나올 예정입니다. 그 뒤를 이어서 PRAX-628과 PRAX-562가 임상2상에 진입해 있습니다. 최근 PRAX-629의 결과가 아주 좋게 나왔습니다.
Praxis Precision Medicines has recorded a midphase win in epilepsy, linking the high dose of PRAX-628 to a 100% complete response rate to clear the path for a larger study in the second half of the year.
The phase 2a trial tested the sodium-channel drug candidate in epilepsy patients with photoparoxysmal response (PPR), a form of photosensitivity. Patients needed to have demonstrated PPR during screening to be evaluated in the trial. After treatment with PRAX-628, Praxis saw a 100% complete response rate in the high, 45mg cohort. The complete response rate on the lower dose was 80%.
Shares in Praxis rose 25% to almost $64 in the opening hours of trading on Tuesday from a Monday closing price of $50.58.
On a conference call with investors to discuss the results, Dan Friedman, M.D., professor of neurology at NYU Grossman School of Medicine, said the photoparoxysmal model is very useful for first-in-patient studies because “it has predictive ability for drugs that are ultimately efficacious in the clinic, especially those with broad spectrum activity.” Friedman cited cenobamate, brivaracetam and levetiracetam as molecules that suppressed PPR and were then shown to be efficacious.
Yet, it is unclear exactly what the effect on PPR means for the prospects of PRAX-628. Friedman said the field lacks “a really good relationship between the degree of suppression we see in these relatively small studies with a heterogeneous group of patients with a specific type of epilepsy, usually a generalized epilepsy, and ultimate efficacy in the clinic.”
45mg 환자들에서 8명중의 8명 (100%)의 Complete Response를 얻었다고 발표를 했습니다. 아직 환자수가 많지 않아서 계속 기대를 가지고 지켜볼 필요가 있습니다.
12학년의 마지막도 거의 다가오고 그래서 그런지 딸아이가 학교 생활로 전보다 더 바빠진 것 같다. 고학년이라 후배들에게 자리를 넘겨주어야 할 것도 있고 학교에서 이런저런 행사들도 준비해야 하는 모양이다.
뿐만 아니라 수업도 마친 것이 아니어서 공부 강도도 이전과 크게 달라진 것이 없는 눈치이다. 매주 시험이 꼭 한두 과목씩 있었는데 다행히 이번주는 시험이 없다고 한다.
오늘은 막내와 함께 어느 대학교의 합격자 설명회를 갔다. 본래 서부에 있는 학교인데 동부 보스턴까지 와서 하는 걸보니 학교 입시 담당자의 마음도 바쁜 모양이다. 6:30에 시작한다고 해서 저녁을 제공하는지 안하는지 도무지 알 길이 없어서 일찍 저녁식사를 하고 갔는데 도착해 보니 만찬이 준비되어 있었다.
딸아이와 나는 서로 바라보면서 피식 웃었다.
학교 행사는 나무랄데 없이 좋았다. 역시 좋은 학교인 것은 틀림이 없다. 학교 소개에 유명인사의 이름과 중요한 사건들, 수많은 노벨상 석학들의 이름이며….스포츠는 또 얼마나 좋고 학교 음식도 좋다고 하고…
뭐 하나 빠지는 법이 없다.
이런 학교에 합격했다는 걸 깨달으며 설명하는 스크린을 바라보고 있자니 갑자기 마음 속에서 울컥하며 이런 생각이 든다.
‘나도 만약 이런 대학 생활을 했다면 얼마나 좋았을까?’
난 사실 고3이 되던 해 1월에 아버지 회사가 부도가 나는 바람에 그 이후부터 대학에 간다는 것보다는 가지 못한다는 마음에 95% 이상은 포기한 상태로 고3 한 해를 보냈었고 대학에 갈 때도 돈을 생각하지 않을 수 없었다. 등록금이 지금 생각해 보면 그리 비쌌던 것도 아닌 듯한데 그 때는 너무나 커 보였다.
어찌어찌 하여 대학에는 갔지만 순탄치 않은 4년이었고 기억하기 싫은 4년이었다. 그래서 지금도 나에게 대학생활은 그리운 시절이 아니라 고달픈 아픔이 되었다.
학교 설명을 들으며 가만히 아이의 옆모습을 보고 있자니 이 녀석…피곤하다고 하면서도 열심히 듣는 모습이 기대에 가득찬 모습이 완연하다.
(Picture: Josep Bassaganya-Riera, Professor of Virginia Tech University, PhD, Founder of Landos Biopharma, Founder & CEO of NImmune Biopharma)
안녕하세요 보스턴 임박사입니다.
바이오텍의 성공확률이 높지 않다는 것은 놀라운 사실이 아니지만 파이프라인에 문제가 없는데도 이사회와의 갈등으로 어려움을 겪는 것은 좀 드문 경우입니다. Virginia Tech 교수이면서 LANCL2 (Lanthionine Synthetase C-Like Protein 2) 라는 표적을 발견하고 이 표적을 이용한 자가면역질환 (Autoimmune Disease) 치료제를 개발하고자 하는 노력에 대해 좀 나누고자 합니다.
Josep Bassaganya-Riera 교수는 2012년에 LANC:2 표적 약물을 Computational Discovery를 통해서 발견했다고 PLOS One에 발표하였습니다.
Landos Biopharma, Inc., an emerging biopharmaceutical company focused on developing improved treatments for autoimmune diseases, announced today it has raised $10 million in a Series A financing led by life sciences investment management firm Perceptive Advisors, LLC, which will serve as its exclusive investor for the Series A round.
Landos, founded by serial entrepreneur and innovator Dr. Josep Bassaganya-Riera, is advancing a robust pharmaceutical pipeline for autoimmune diseases toward commercialization and will partner operational efforts with Xontogeny, LLC, a life sciences accelerator operating company led by industry veteran Chris Garabedian. Xontogeny’s model works in synergy with partner companies to support management teams and provide expertise and strategic direction in the early stages of pharmaceutical and biotechnology development.
Current therapies for autoimmune diseases, a $100 billion market, have limited efficacy and significant side effects. Landos’ mission is to accelerate the development of safer, more effective therapeutics for painful and debilitating autoimmune diseases including Crohn’s disease and ulcerative colitis.
“I’m thrilled to have Xontogeny and Chris Garabedian as a strategic and operating partner along with Perceptive Advisors as Landos’ exclusive financier in the Series A, to bring our lead product, BT-11, through initial clinical studies in 2018,” said Landos Chairman and CEO, Dr. Josep Bassaganya-Riera “We have a committed leadership team with industry experience focused on developing oral treatments that address an unmet clinical need of patients, can disrupt the $9.2 billion per year inflammatory bowel disease (IBD) therapeutics market, and most importantly improve the lives of millions of patients living with these diseases.”
Landos will focus its development efforts in a novel target pathway called Lanthionine Synthetase C-Like 2 (LANCL2), which has shown promise for the treatment of autoimmune diseases by engaging a unique mechanism of action that exerts potent anti-inflammatory effects. Landos’ lead product candidate BT-11 is a first-in-class, orally active, locally-acting therapeutic for treatment of Crohn’s disease and ulcerative colitis that has shown a benign safety profile in animal models and that is advancing toward an Investigational New Drug (IND) filing. BT-11 intercepts IBD by decreasing the production of inflammatory mediators and increasing anti-inflammatory molecules within the gastrointestinal tract. IBD impacts approximately 1.6 million Americans and 4 million people worldwide.
“Landos is an exciting company for Xontogeny to partner with as Josep and his team have produced very compelling data in animal models of IBD and have brought their lead compound, BT-11, to the cusp of clinical trials,” said Mr. Garabedian, who will serve as a Landos Board member and senior business advisor. “The properties of BT-11 are unique and well differentiated from current IBD products and we believe it has the potential to represent an advance in the treatment of both Crohn’s disease and ulcerative colitis.”
“We are extremely excited to partner with both Josep and Chris to build Landos into a global biopharmaceutical company focused on autoimmune diseases, and are convinced that the team will provide an accelerated path to compelling clinical proof-of concept for IBD,” said Joe Edelman, CEO of Perceptive Advisors. “As the first investment in a Xontogeny portfolio company since partnering with Chris earlier this year, we believe that Landos exemplifies the company profile we aim to support – an outstanding leadership team, a lead product with a novel mechanism, strong IP, and a compelling preclinical and translational dataset that is close to the clinic for the treatment of an important disease with an unmet need for safer and more effective drugs.”
With the Series A investment, Landos plans to complete remaining IND-enabling studies, file an IND for BT-11 in 2018 and expects to complete Phase 1 clinical testing by early 2019.
Landos Biopharma, Inc. is an emerging biopharmaceutical company focused on the discovery and development of first-in-class oral therapeutics for patients with autoimmune diseases. Landos’ lead clinical asset, BT-11, is a novel, locally-acting small molecule targeting inflammatory bowel disease (IBD) that is expected to enter clinical testing for Crohn’s disease in 2018. Landos also has a robust pipeline of compounds for other autoimmune diseases. Landos is headquartered in Blacksburg, VA. For more information, please visit www.landosbiopharma.com, contact info@landosbiopharma.com or follow the company on Twitter at @LandosBio.
Two years ago, Landos Biopharma was the first biotech to come out of Xontogeny, the accelerator started by former Sarepta Therapeutics chief Chris Garabedian. Now, the autoimmune specialist has picked up $60 million to propel its lead program into phase 2 for inflammatory bowel disease (IBD).
The series B funding will also advance Landos’ earlier-stage pipeline, which includes candidates slated to enter the clinic in 2020. It comes from RTW Investments, Osage University Partners, PBM Capital and Perceptive Advisors—which includes Perceptive Life Sciences Fund and Perceptive Xontogeny Venture Fund.
Landos is based upon the work of CEO Josep Bassaganya-Riera, Ph.D., a serial entrepreneur and Virginia Tech professor who outlined the potential for targeting the lanthionine synthetase c-like protein 2 (LANCL2) pathway to affect immune and inflammatory responses in a 2014 paper. Bassaganya-Riera went on to discover a drug that selectively binds LANCL2, found Landos and pick up $10 million from Perceptive Advisors to drive its lead program.
The program, dubbed BT-11, is a small molecule that targets LANCL2 in the gut. In a phase 1 study published earlier this year, the drug beat placebo at lowering levels of fecal calprotectin, which Landos believes is a predictive biomarker of response to treatment in IBD. The company will kick off global phase 2 trials in the two main forms of IBD: Crohn’s disease and ulcerative colitis.
“We believe BT-11’s mechanism of action is differentiated with the potential to transform the current treatment paradigm for patients with ulcerative colitis and Crohn’s disease,” said Rod Wong, M.D., a managing partner at RTW Investments who has just joined Landos’ board, in a statement.
Landos is looking to provide a new option for patients with moderate to severe cases of IBD for whom current treatments are inadequate or have side effects. People with IBD may be treated with anti-inflammatory drugs or immunosuppressants such as anti-TNF (tumor necrosis factor) meds, but Landos believes the former can be used only in mild inflammation and reckons the latter only works in up to 60% of patients.
“We believe there is tremendous commercial potential for an oral compound for IBD and BT-11 is the most promising candidate we’ve seen at this stage of development,” said Garabedian, portfolio manager at Perceptive Xontogeny Venture Fund. “As an investor in the Series A, we are impressed with the productivity and efficiency of the Landos team in completing a comprehensive preclinical program, securing two open INDs, and successfully generating Phase 1 clinical results in less than two years, and are prepared to move forward with two global Phase 2 studies in ulcerative colitis and Crohn’s disease.”
그리고 이어서 NX-13이라는 두번째 약물을 임상1상에서 첫번째 환자에게 약물복용이 되었다고 발표를 했습니다. 정말 굉장한 추진력입니다.
Landos Biopharma, a clinical-stage biopharmaceutical company focused on the discovery and development of therapeutics for patients with autoimmune disease, today announced that the first patient has been dosed in a Phase 1 study of NX-13, the Company’s novel, orally administered therapeutic candidate for the treatment of inflammatory bowel disease.
“Today marks a significant milestone for Landos, as we advance our second product candidate, NX-13, into clinical development,” commented Josep Bassaganya-Riera, Ph.D., Chairman, President, and CEO of Landos Biopharma. “This achievement highlights the success of our precision medicine platform in identifying novel targets to establish a robust and differentiated therapeutic pipeline for autoimmune disease. NX-13 is a compound for oral administration that targets the NLRX1 receptor, which is part of a pathway that modulates immune response linked to inflammatory bowel disease. We believe that, if approved, NX-13 could provide an additional treatment option to the up to 50 percent of ulcerative colitis patients that experience relapse within 1 year of current therapies and up to 70-90 percent of Crohn’s disease patients that fail to enter prolonged remission.”
The randomized, double-blind, placebo-controlled, ascending dose, multi-cohort Phase 1 study will evaluate the safety, tolerability, and pharmacokinetics of NX-13 in healthy volunteers. The study design includes evaluation of single ascending doses and multiple ascending doses of NX-13. Based on observations in preclinical models of inflammatory disease, NX-13 has the potential to be developed as a monotherapy or in combination with other therapeutics in the treatment of inflammatory bowel disease.
“Advancing two first-in-class oral products for Crohn’s disease and ulcerative colitis with new mechanisms of action into clinical development in less than 2 years is a substantial accomplishment,” said Jean-Frederic Colombel, M.D., a Clinical Advisory Board member for Landos’ IBD program, gastroenterologist and Director of the IBD Center at the Icahn School of Medicine at Mount Sinai. “We continue to see an unmet clinical need for chronic oral therapies to treat UC and CD with improved efficacy, safety, tolerability and convenience, including in the mild to moderate patients.”
About Inflammatory Bowel Disease
Inflammatory bowel disease (IBD) is a chronic autoimmune disorder with two primary subtypes: Crohn’s disease and ulcerative colitis, which impair quality of life and afflict over five million individuals worldwide.1 Currently, available therapeutics typically are only able to address a subset of overall patient populations and many fail to maintain therapeutic efficacy over time. In addition, current therapeutics are associated with serious side effects and toxicities related to systemic immunosuppression, including increased mortality.2
1. World IBD Day. Home. Available at http://www.worldibdday.org/index.html. Accessed July 2020. 2. Shivaji, U.N. et al., Review article: managing the adverse events caused by anti-TNF therapy in inflammatory bowel disease. Aliment Pharmacol Ther. 2019 Mar;49(6):664-680.
About NX-13
NX-13 is a first-in-class, orally-active, gut-restricted, small molecule therapeutic candidate for the treatment of inflammatory bowel disease. NX-13 targets NLRX1, a mitochondria-associated receptor with the ability to modulate immune responses. By activating the NLRX1 pathway, NX-13 increases oxidative phosphorylation in immune cells, reduces differentiation of effector CD4-positive T cells, and decreases production of inflammatory cytokines.
About Landos Biopharma
Landos Biopharma, Inc. is a clinical-stage biopharmaceutical company focused on the discovery and development of first-in-class oral therapeutics for patients with autoimmune disease. Lead asset BT-11 is a novel, first-in-class, oral, gut-restricted therapeutic candidate for the treatment of ulcerative colitis and Crohn’s disease that targets the LANCL2 pathway. NX-13 is a novel, first-in-class, oral, gut-restricted compound for the treatment of inflammatory bowel disease, which targets the NLRX1 pathway. Additional candidates are in development for the treatment of lupus nephritis, rheumatoid arthritis, multiple sclerosis, and diabetes. For more information, please visit www.landosbiopharma.com.
그리고 이듬해에는 $100 Million IPO를 할 수 있었습니다. 여기까지는 모든 것이 다 좋아보였습니다.
Xontogeny’s Landos Biopharma is jumping into warm biotech IPO waters as it looks to go public with a $100 million offering.
Landos is based upon the work of CEO Josep Bassaganya-Riera, Ph.D., a serial entrepreneur and Virginia Tech professor who outlined the potential for targeting the lanthionine synthetase c-like protein 2 (LANCL2) pathway to affect immune and inflammatory responses in a 2014 paper.
Bassaganya-Riera went on to discover a drug that selectively binds to LANCL2, found Landos and pick up $10 million from Perceptive Advisors to drive its lead program.
Landos Biopharma was the first biotech to come out of Xontogeny, the accelerator started by former Sarepta Therapeutics chief Chris Garabedian. Back in the summer of 2019, it picked up $60 million series B to propel its lead program into phase 2 for inflammatory bowel disease (IBD).
Now, it wants a $100 million IPO, according to its Securities and Exchange Commission filing, to help boost its AI-based LANCE platform, which sees to make predictions of immunometabolic function. To date, it has identified seven novel immunometabolic targets and product candidates across 14 indications.
Its leading candidate, BT-11, has completed the induction phase of a phase 2 trial in mild to moderate ulcerative colitis (UC) patients, with plans to kick-start a phase 3 in UC and a phase 2 for moderate to severe Crohn’s disease in the coming months.
Landos is looking to provide a new option for patients with moderate to severe cases of IBD for whom current treatments are inadequate or have side effects.
People with IBD may be treated with anti-inflammatory drugs or immunosuppressants such as anti-TNF meds, but Landos believes the former can be used only in mild inflammation and reckons the latter only works in up to 60% of patients. It will now seek to out that theory to the test in later-stage trials.
그런데 IPO한 지 얼마되지 않아 Josep 교수는 갑자기 회사를 그만두게 됩니다. 이사진과의 갈등이 원인이 된 것 같죠. 아마 주된 이유는 이후의 일로 보았을 때 BT-11과 NX-13 중에서 어떤 약물을 집중하느냐의 문제였던 것으로 보입니다. Josep 교수가 그만둔 후 Landos는 NX-13의 임상을 진행하고 BT-11은 중단합니다.
Josep Bassaganya-Riera, chief executive of Landos Biopharma, leaves. As announced by Landos Biopharma Inc. in a news release on Monday, November 8, 2021, Josep Bassaganya-Riera leaves his post as chief executive officer at the clinical-stage biopharmaceutical company, after about five years in the role, effective immediately.
Landos Biopharma will undertake a search for a successor.
Josep Bassaganya-Riera’s duties as CEO will be taken over temporarily by Tim M. Mayleben, most recently President, CEO and Director at Esperion Therapeutics, Inc., as Interim Chief Executive Officer.
Already a director
Mayleben is already a director of Landos Biopharma. Generally speaking, most director-turned-CEO appointments occur following a sudden resignation of the outgoing CEO and signal a lack of preparedness on the company’s part to groom internal talent. Directors-turned-executives represent a blend of outsider and insider.
They don’t have the constraints of a pure insider when it comes to leading painful changes or making unpopular decisions, and they have more company knowledge than a pure outsider.
Having been a director, Mayleben understands the expectations and dynamics of the board and has knowledge of Landos Biopharma’s organization, risk-management practices and strategy.
Chris Garabedian, also a Landos Director, has been appointed Chairman of the Board.
“This is the right time”
Josep Bassaganya-Riera’s departure from the CEO post is explained as follows. Chris Garabedian, Chairman of the Board, said: “With seven product candidates in the pipeline across three novel mechanisms, Josep and the Board agree that this is the right time to transition to our next phase of leadership.”
Precise information regarding Josep Bassaganya-Riera’s future plans was not immediately available.
“Stepped down”
Landos Biopharma said: “Josep Bassaganya-Riera, Ph.D., has stepped down as Chairman, President and Chief Executive Officer, effective immediately.”
Share price increase since June 2021
The announcement follows an increase in Landos Biopharma Inc.’s share price of 30% since June 2021.
In the position of CEO since 2017
Josep Bassaganya-Riera became CEO of the Company in 2017.
Bassaganya-Riera will serve as an advisor to the Company to ensure a smooth transition.
Josep Bassaganya-Riera has served as the Company’s Chairman, President and Chief Executive Officer since the Company’s founding in January 2017.
Bassaganya-Riera has served as the Director of the Nutritional Immunology and Molecular Medicine Laboratory since July 2002 and the Chairman of the board of directors of Biotherapeutics Inc. since October 2008.
He previously served as the Chief Executive Officer of Biotherapeutics from October 2008 to September 2017 and a Research Professor of Immunology at Virginia Tech from December 2002 to May 2020.
Bassaganya-Riera holds a degree in Veterinary Medicine from Universitat Autònoma de Barcelona and a Ph.D. in Nutrition and Immunology from Iowa State University.
하지만 Josep 교수는 여기서 포기하지 않습니다.2023년 3월에 Landos로 부터 NX-13을 제외한 물질을 사게 됩니다. 그리고 NImmune Biopharma를 설립합니다.
Endpoints 의 기사가 좀더 자세히 상황을 설명해 주는 것 같습니다. 약물의 용량을 줄이고 subset disease로 임상3상을 추진한다는 계획을 밝혔습니다. 펀딩에 대해서는 자세한 언급은 없었지만 투자자들이 든든히 받치고 있다고 했다는군요. 펀딩 부분은 조만간 뉴스가 있겠죠.
By the time Josep Bassaganya-Riera stepped down as founding CEO of Landos Biopharma in 2021, the company had racked up Phase II data for its top autoimmune program, completed what he called a positive end-of-Phase-II meeting with the FDA and plans to launch pivotal Phase III trials.
Since then, though, the new leaders at Landos have reshuffled their plans for the drug, omilancor, first announcing they will run a Phase IIb ahead of a Phase III and eventually shelving it altogether.
Now, Bassaganya-Riera is picking back up where he left off.
NImmune Biopharma, his new startup, has bought rights to omilancor and other similar drugs from Landos, with an eye to launching Phase III this year. The company’s name first cropped up in SEC filings when Landos announced the deal in early March, but Bassaganya-Riera is sharing more details about the Phase III design and his team in an official launch.
Joining him in the C-suite are several veterans of Landos, including CSO Raquel Hontecillas, Marek Ciszewski (CFO), Andrew Leber (chief development officer), and Jennifer Collette (chief accounting officer & controller). The executives were formerly Landos’ VP of financial strategy and investor relations, VP of scientific & product development and head of finance, respectively.
The team’s focus remains on a portfolio of drugs targeting LANCL2, a protein that Bassaganya-Riera had researched for years as a professor at Virginia Tech.
While the clinical remission rate shown in the Phase II trial Landos ran in mild-to-moderate ulcerative colitis was not statistically significant, Bassaganya-Riera believes there’s evidence the drug works for a subset of patients with more serious disease.
For the late-stage trial, that means “a refinement of the patient population consistent with the expectations of the FDA.”
“In a nutshell, the expectation of the FDA is that we focus on patients that have more active disease,” he said, adding that NImmune will go for a 440 mg dose, which is lower than the 500 mg and 1,000 mg tested in Phase II.
He declined to offer specifics on fundraising progress so far, saying only there are institutional investors on board that will put NImmune in a well-capitalized position.
NImmune will aim to start other trials for omilancor in Crohn’s disease while testing a second candidate for lupus and rheumatoid arthritis — in line with the broad potential it sees for the LANCL2 pathway in treating autoimmune diseases.
“It’s different from the current Landos, but it’s not that different from the Landos that I founded in 2017,” he said.
NImmune Biopharma (“NImmune”), a late-stage precision immunology biopharmaceutical company that develops best-in-class biomarker-driven immunoregulatory therapeutics, today announced its launch following the acquisition of omilancor, NIM-1324, and the entire LANCL portfolio of immunoregulatory therapeutic assets from Landos Biopharma, Inc.
Omilancor is a Phase-3-ready, once-daily, oral, gut-restricted therapeutic for Ulcerative Colitis (UC) with potentially fast-to-market follow-on opportunities in Crohn’s disease (CD) and Psoriasis. NIM-1324 is a Phase-2-ready biomarker-guided once-daily, oral therapeutic for the treatment of Systemic Lupus Erythematosus (SLE) and Rheumatoid Arthritis (RA). These clinical candidates, originally developed by NImmune’s Founder, Executive Chairman, President, and Chief Executive Officer Dr. Josep Bassaganya-Riera, activate the Lanthionine Synthetase C-Like 2 (LANCL2) pathway, which enhances immunoregulatory processes that provide protection from autoimmune disease.
“I am thrilled to regain ownership and leadership of the LANCL immunoregulatory therapeutic portfolio and look forward to continuing the development of these candidates at NImmune, a science-driven company developing best-in-class biomarker-driven immunoregulatory therapeutics for a growing patient population with autoimmune diseases and unmet medical needs,” stated Dr. Bassaganya-Riera, Founder & CEO of NImmune. “Our leadership team was instrumental in the creation of the LANCL immunoregulatory portfolio, and brings substantial experience working with omilancor specifically to NImmune. Omilancor has the potential to impact the global inflammatory bowel disease (IBD) market as a safe and effective therapy, given the statistically significant clinical remission data it has produced in active disease UC patients as well as promising efficacy and safety results in CD patients. We are highly encouraged and motivated by these results and are pleased to have identified a robust regulatory path to commercialization.”
Omilancor was previously evaluated for the treatment of UC in a Phase 2 randomized, placebo-controlled clinical trial that demonstrated biologic-like efficacy with potentially best-in-class safety. Based on these findings and positive correspondence with the U.S. Food and Drug Administration (FDA), NImmune plans to initiate a Phase 3 randomized, placebo-controlled clinical trial in 2023. This study will be similar in design to the previous study but will only include the 440mg dose and utilize refined criteria for active disease, that includes rectal bleeding (RB) > 0, histological activity and elevated fecal calprotectin (FCP) at baseline. An analysis of the Phase 2 data using the 440mg dose and the refined active disease population attained statistically significant clinical remission at week 12. Meeting the approvable primary endpoint in its planned Phase 3 population of active disease UC patients sets a robust regulatory path for omilancor to New Drug Application (NDA) filing and commercialization.
A summary of the Phase 2 omilancor data can be found in NImmune’s corporate presentation.
NImmune’s second pipeline clinical candidate, NIM-1324, a once-daily, oral, systemically distributed LANCL2 agonist, has demonstrated ability to induce enhanced regulatory T cell (Treg) function in preclinical models of SLE and RA, reduced interferon gamma signaling in human peripheral blood mononuclear cells, and the potential to reduce inflammatory cell infiltration with less toxicity than current standard of care, including biologics and JAK-inhibitors. Additionally, Phase 2-ready NIM-1324 successfully completed a Phase 1 randomized, double-blind, placebo-controlled multi-cohort study evaluating its safety, tolerability, and pharmacokinetics (PK) in normal healthy volunteers where all endpoints were met, and it is now ready for further clinical testing in lupus and RA patients.
About NImmune Biopharma
NImmune is a late-stage precision immunology biopharmaceutical company that develops best-in-class biomarker-driven immunoregulatory therapeutics. Underpinned by advanced computational modeling and bioinformatics coupled with biomedical research capabilities to pioneer innovation in immunoregulatory drug development, NImmune’s business model enables the rapid and capital-efficient clinical development of high conviction drug candidates into New Drug Application (NDA) filing and commercialization. NImmune’s clinical development pipeline includes omilancor, a Phase 3-ready lead clinical candidate targeting LANCL2, an oral, once-daily, gut-restricted, first-in-class therapeutic for Ulcerative Colitis and Crohn’s disease with registration-directed pivotal clinical trials planned for 2023. Additional information: www.NIMMUNEBIO.COM or contact media@nimmunebio.com.
NImmune Biopharma, (“NImmune”), a private late-clinical-stage precision immunology biopharmaceutical company focused on the discovery and development of best-in-class biomarker-driven immunoregulatory therapeutics, led by omilancor, a Phase 3 best in class once daily oral therapy for Ulcerative Colitis, announced that it will present three abstracts, including final Phase 2 data for omilancor in active Ulcerative Colitis patients at the American College of Gastroenterology (“ACG”) 2023 Annual Scientific Meeting (“ACG 2023”), taking place at the Vancouver Convention Center in Vancouver, Canada, between October 20 and October 25, 2023.
Dr. Josep Bassaganya-Riera, Founder & CEO of NImmune, said, “Final and complete Phase 2 data for omilancor in mild to severe UC patients with active disease affirms best-in-class efficacy and unrivaled safety. Omilancor is a first-in-class wholly-owned therapeutic, developed with the guidance of TITAN-X, a proprietary computational modeling and AI-powered precision medicine discovery engine that efficiently accelerates biomarker-driven immunoregulatory therapeutic development of omilancor, NIM-1324 and our other immunoregulatory therapeutics. Meeting the primary endpoint of clinical remission in UC patients with active disease substantially de-risks omilancor’s regulatory path to New Drug Application (NDA) and commercialization and provides clinical validation of the LANCL2 pathway as a novel mechanism of action for addressing the significant unmet clinical needs of patients with autoimmune diseases. These positive clinical findings further underscore the importance of our recently announced research collaboration with the NIMML Institute and the value of its advanced computational modeling and A.I.-powered TITAN-X precision medicine platform, which efficiently accelerates biomarker-driven immunoregulatory therapeutic development of omilancor, NIM-1324 and our other immunoregulatory therapeutics.”
“As we approach a significant milestone—the initiation of the pivotal global Phase 3 clinical program of omilancor for the treatment of UC by year-end 2023—we are pleased to present our results at ACG 2023 and encouraged by the continued scientific validation of our clinical findings and the overall momentum of omilancor’s clinical and regulatory development. We look forward to continuing to realize the significant potential of omilancor as the first-in-class LANCL2 agonist for UC and additional autoimmune indications including Crohn’s disease and psoriasis.”
Presentation Details
Title: Efficacy and Safety of Omilancor in a Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial of Patients with Ulcerative Colitis.
Poster: Board NumberP2216,Monday October 23, 2023, 10:30 AM – 4:15 PM
Clinical remission in the approvable UC population of active disease mild to severe patients was induced in 30.4% of patients treated with omilancor relative to 3.7% of patients given placebo (Δ=26.7, P = 0.01), meeting the primary endpoint.
Endoscopic and histological remission were achieved in 41.7% of omilancor given patients relative to 18.6% and 22.2%, respectively, patients in the placebo group (Δ=23.1, Δ=19.5).
Durable remission was induced in 38.5% of patients in the omilancor group versus 21.4% of patients given placebo (Δ=17.1, P = 0.05).
Endoscopic response was achieved in 73.1% of patients treated with omilancor relative to 53.6% of patients given placebo (Δ = 19.5, P = 0.02).
Omilancor exhibited statistically significant decreases in TNF-a expressing myeloid cells (p = 0.037) in the colonic mucosa and statistically significant normalization of fecal calprotectin levels (P = 0.048).
Oral omilancor was well-tolerated in patients with UC with no trends in AE profile observed and no dose-limiting toxicities.
Pharmacokinetic analysis validated a gut-restricted profile with stable drug levels in stool over the treatment period, penetration into colonic biopsy tissue and limited systemic exposure.
Title: Efficacy and Safety of Omilancor in a Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial of Patients with Crohn’s Disease.
Poster: Board NumberP2215,Monday October 23, 2023, 10:30 AM – 4:15 PM
PRO-2 clinical remission was achieved in 41.7% of moderate to severe CD patients in the omilancor group relative to 9.1% give placebo (Δ=32.6).
Crohn’s disease activity index (CDAI) clinical remission was achieved in 25.0% of omilancor-treated patients relative to 9.1% of the placebo group (Δ=15.9).
Omilancor demonstrated a promising efficacy signal in both biologic naïve and biologic-experienced moderate to severe CD patients.
Normalization of fecal calprotectin was induced in 33.3% of patients treated with omilancor compared to 14.3% in the placebo group (Δ=19.0).
In patients with histological activity in at least one segment at baseline, omilancor induces remission in all segments in 42.9% of patients relative to 20.0% in the placebo group (Δ=22.9).
Oral omilancor was well tolerated in patients with CD and displayed a benign safety profile.
Title: Transcriptional Analysis of Colonic Biopsies from Patients with Ulcerative Colitis Treated with Omilancor.
Poster: Board NumberP2217, Monday October 23, 2023, 10:30 AM – 4:15 PM
Predictive biomarker signatures from colonic biopsies were identified by using the RandomForest A.I. algorithm within NIMML’s TITAN-X drug development platform.
A newly identified precision immunology biomarker signature predicts omilancor responders from non-responders with 75% accuracy and patients treated with omilancor and achieving clinical remission were identified with 100% accuracy.
Predictive modeling of gene expression changes from baseline accurately differentiated patients treated with omilancor from those given placebo with 83% accuracy.
Biomarkers upregulated by omilancor were associated with lipid metabolism, ion balance, and known critical elements of the LANCL2 pathway.
Biomarkers downregulated by omilancor were associated with immune systems processes, mainly linked to neutrophils and leukocyte trafficking.
The posters will be available under the “Publications” section of the NIMML’s website at www.nimml.org and at the ACG 2023 ePoster Hall during and after the meeting. Additionally, the peer-reviewed accepted abstracts will be published verbatim in a special supplement to the October 2023 issue of The American Journal of Gastroenterology.
About Ulcerative Colitis (UC) UC is a chronic, autoimmune, inflammatory bowel disease that causes inflammation, irritation, and ulcers in the lining of the large intestine (colon) and rectum. Symptoms include abdominal pain, rectal pain and bleeding, bloody stools, diarrhea, fever, weight loss, and malnutrition. Having UC puts a patient at increased risk of developing colon cancer. Diagnosis typically occurs in early adulthood and the disease requires maintenance treatment for the remainder of the patient’s life. UC is estimated to affect over 900,000 patients in the United States and over 1 million patients throughout the rest of the world. With 70% of addressable patients experiencing a second flare within one year and 30% of patients in remission failing to stay in remission for more than one year, there is an unmet medical need in UC for safer and more efficacious therapeutics.
About Crohn’s Disease (CD) CD is a chronic, autoimmune, inflammatory bowel disease that causes inflammation, irritation and ulcers in any segment of the gastrointestinal tract. CD impacts the end of the small bowel and beginning of the colon most commonly, which in turn can lead to symptoms of abdominal pain, increased abdominal sounds, rectal pain and bleeding, bloody stools, diarrhea, fever, weight loss and malnutrition. There are four classes of CD and treatment depends on the level of severity. Current therapeutic options for severe disease, primarily biologics, have several limitations, which include but are not limited to safety risks for malignancies and infections, limited efficacy and lack of long-term maintenance options. There is an urgent need to establish a consensus for a first-line therapy for CD and improve upon the existing constraints in administration and efficacy.
About Omilancor By activating the LANCL2 pathway and modulating the interactions between immunological and metabolic signals in immune and epithelial cells, omilancor is a first-in-class, oral, once-daily, gut restricted therapeutic designed to create a favorable regulatory microenvironment in the gut, decreasing the production of key inflammatory mediators and increasing anti-inflammatory functions in regulatory T cells (Treg) within the site of inflammation. Omilancor has completed Phase 2 clinical testing in UC patients showing a clinical remission of 30.4% with a placebo-adjusted 12-week clinical remission rate of 26.7% (p=0.01) for the 440 mg dose. Following demonstration of a statistically significant approvable primary endpoint for clinical remission in an active disease patient population, NImmune expects to initiate a global pivotal Phase 3 program (PACIFY I and PACIFY II trials) in UC patients in the second half of 2023. Omilancor’s target U.S. market size is expected to be valued at $394.9 billion 2021-2030, of which a peak annual market size of $49.5 billion is expected to occur in 2030. NImmune expects peak unadjusted revenue of $12.5 billion in 2030.
About NIM-1324 NIM-1324 is an oral, systemically distributed, small-molecule therapeutic candidate which activates LANCL2, a surface membrane-associated receptor that is responsible for modulating key cellular and molecular changes tied to autoimmune diseases. By activating the LANCL2 pathway, NIM-1324 increases the anti-inflammatory capacity and stability of regulatory CD4+ T cells while also supporting the metabolic demands of autophagy in phagocytes. To date, treatment with NIM-1324 has reduced the production of interferon alpha in human peripheral blood mononuclear cells (PBMCs) from systemic lupus erythematosus (SLE) patients and provided protection from clinical disease and tissue pathology in mouse models of lupus, rheumatoid arthritis, and multiple sclerosis. Phase 2-ready NIM-1324 completed Phase 1 clinical testing where it met all endpoints and demonstrated a dose proportional change in plasma exposure within the therapeutic range with no accumulation.NIM-1324 target U.S. market size is expected to be valued at $226.0 billion 2021-2030, of which a peak annual market size of $23.1 billion is expected to occur in 2030. NImmune expects unadjusted revenue estimates from NIM-1324 therapeutics to be valued at $2.3 billion from the 2028-2030 projections.
About NImmune Biopharma NImmune is a late-stage precision immunology biopharmaceutical company that develops novel best-in-class biomarker-driven immunoregulatory therapeutics. Underpinned by a discovery platform that utilizes advanced computational modeling, A.I. and bioinformatics coupled with biomedical research capabilities to pioneer innovation in immunoregulatory drug development, NImmune’s business model enables the rapid and capital-efficient clinical development of high conviction drug candidates into New Drug Application (NDA) filing and commercialization. The lead product candidate from NImmune’s internal discovery platform is omilancor, a wholly-owned Phase 3 oral, once-daily, gut-restricted, first-in-class therapeutic targeting LANCL2 for Ulcerative Colitis, with fast follower potential in Crohn’s disease, Psoriasis and other autoimmune diseases. Phase 2 first-in-patient data for omilancor in UC show potential best in class efficacy and safety. To learn more, visit www.NIMMUNEBIO.COM or contact media@nimmunebio.com.
그러는 와중에 Landos Biopharma는 $138 Million에 Abbvie에 팔렸습니다. 신약개발은 개발자의 의지와 추진력이 중요한데 Josep 박사가 이끄는 팀의 추진력이 매우 좋고 의지도 좋습니다. 몇년간의 마음고생이 있었겠지만 다시 일어난 만큼 좋은 결과가 있기를 진심으로 기대해 봅니다.
AbbVie has grabbed a wrench to add on some new autoimmune disease options to its pipeline via the acquisition of Landos Biopharma.
The deal values the oral-therapeutic-focused biotech at $137.5 million, with the terms offering $20.42 per share in cash upon closing. AbbVie is also offering a non-tradeable contingent value right at up to $11.14 per share, or an additional $75 million, subject to certain clinical milestones.
AbbVie’s business development team has been incredibly busy over the past few months, snapping up Cerevel Therapeutics in neuroscience and ImmunoGen in oncology for $8.7 billion and $10.1 billion, respectively. But that left immunology, where AbbVie has a major legacy thanks to Humira that just went off patent.
Executives previewed a plan to look for smaller companies after those major outlays, with President and Chief Operating Officer Robert Michael saying that the team would be on the lookout for some smaller deals with early-stage opportunities. Michael said during a fourth-quarter earnings call in February that “our focus in immunology in terms of BD is really looking for new mechanisms of action that can elevate standard of care, whether monotherapy or in combination. I’d say there’s a lot of interest in combination.”
Landos will bring the phase 2 asset NX-13 to the mix, an oral NLRX1 agonist with a bimodal mechanism of action that acts as an anti-inflammatory by facilitating epithelial repair. The biotech is evaluating the treatment in the midstage NEXUS trial in patients with ulcerative colitis (UC). Top-line data are expected in the fourth quarter, according to Landos’ fourth-quarter earnings update issued last week. In addition, NX-13 is being prepped for a phase 2 test in Crohn’s disease.
Also in the pipeline at Landos for the NLRX1 pathway is LABP-66 in multiple sclerosis and other neurodegenerative diseases, plus LAPB-73 in asthma and eosinophilic disorders. The company is studying the PLXDC2 pathway with the early-stage med LABP-69 in rheumatoid arthritis, UC and Crohn’s.
The transaction is expected to close in the second quarter.
 Productive Longevity: What can Work in Low- and Middle-Income Countries? – World Bank Policy Research Working Paper")
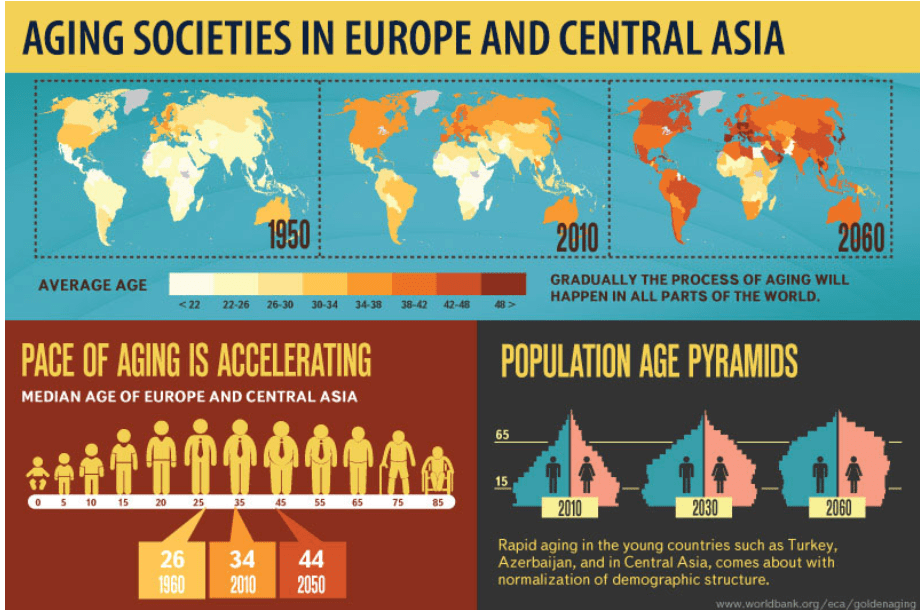


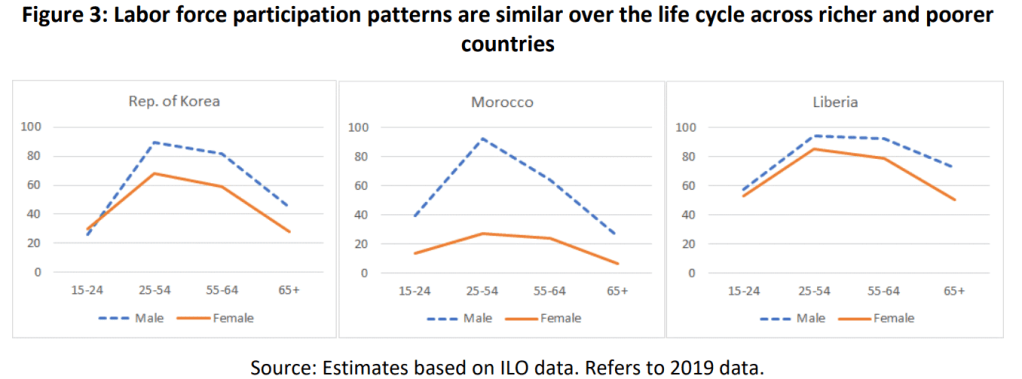
 손석희 아나운서")

 Xilio Therapeutics: Tumor-Activated Immuno-Oncology")

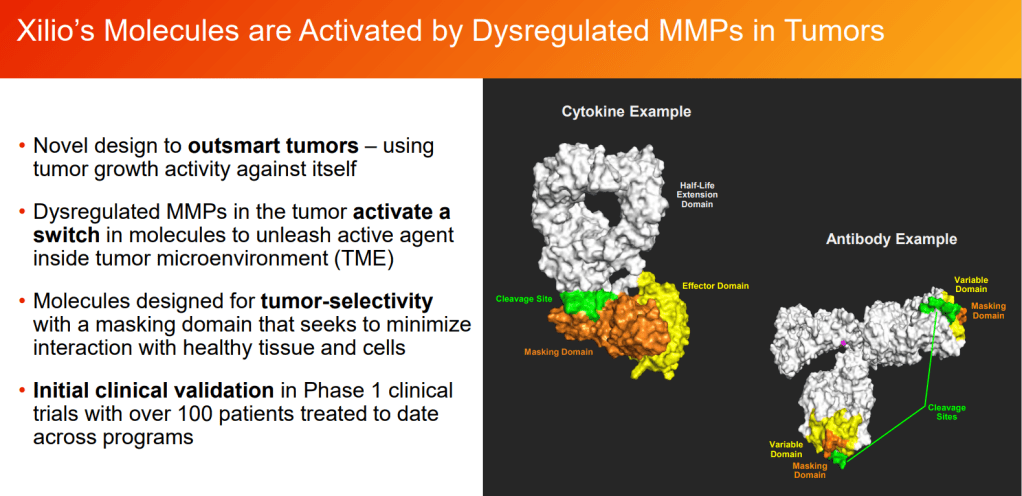

 Aging Asia rethinks retirement to pursue ‘productive longevity’ – Nikkei Asia")


 Singaporeans attend a job seminar organized by the Center For Seniors on June 10. (Photo by Kentaro Iwamoto)
Singaporeans attend a job seminar organized by the Center For Seniors on June 10. (Photo by Kentaro Iwamoto)
 The Japanese government wants large corporations to do more to carry the burden of the aging society and swelling pension outlays. (Photo by Hideki Yoshikawa)
The Japanese government wants large corporations to do more to carry the burden of the aging society and swelling pension outlays. (Photo by Hideki Yoshikawa)
 Managing Oneself by Peter F. Drucker, PhD.")

 Avenzo Therapeutics: Turning Point Therapeutics Reunion – Acquisition of Early-Stage Oncology Small Molecules, ADCs from Chinese Biotech & US Biopharma")

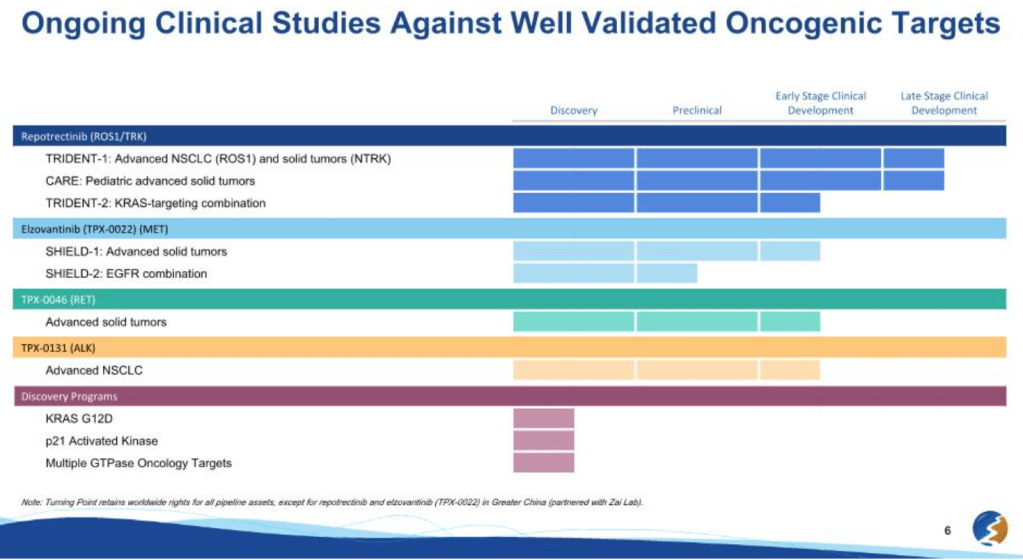
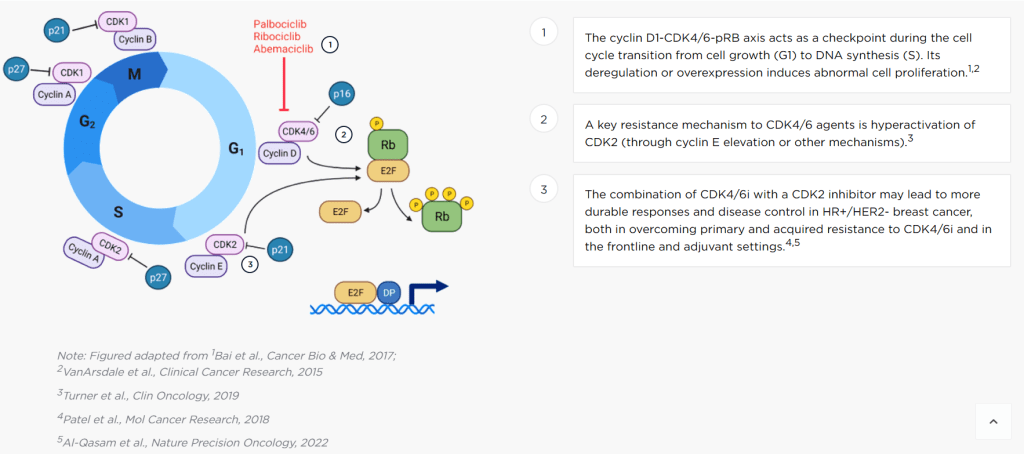

 Praxis Precision Medicines: CNS Small Molecules & Antisense Oligonucleotides Platform")

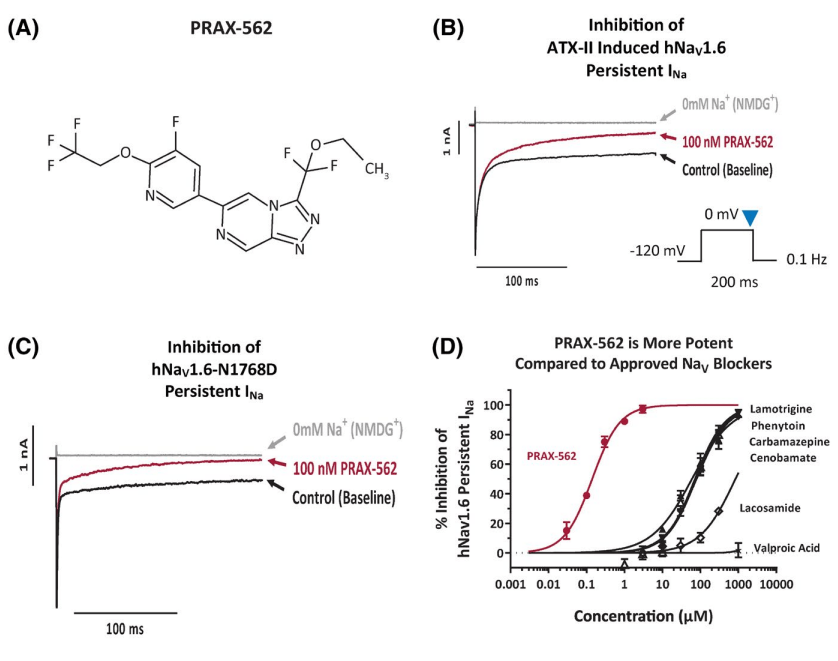
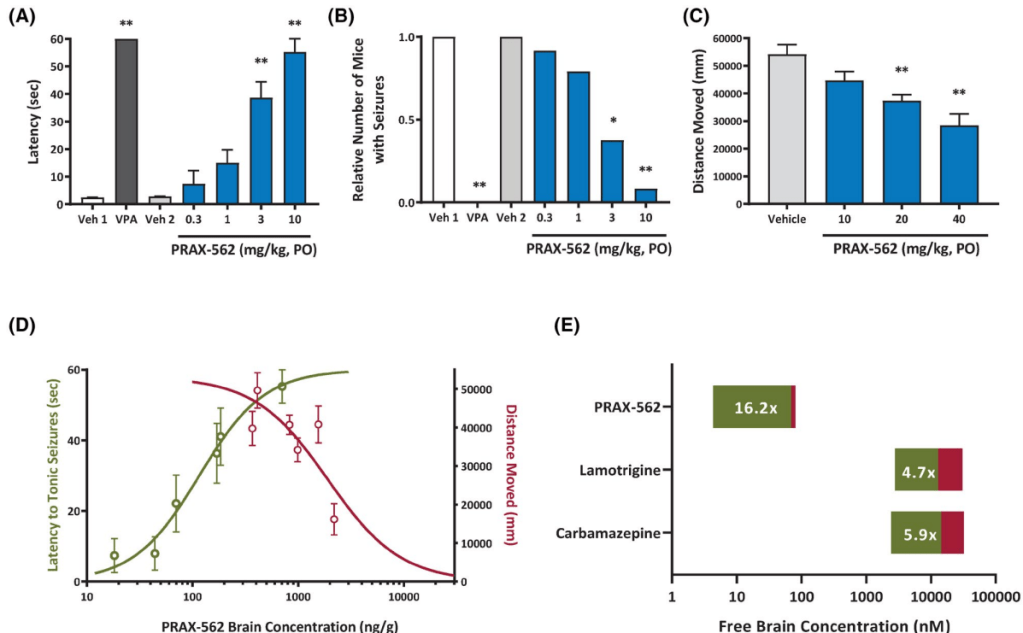
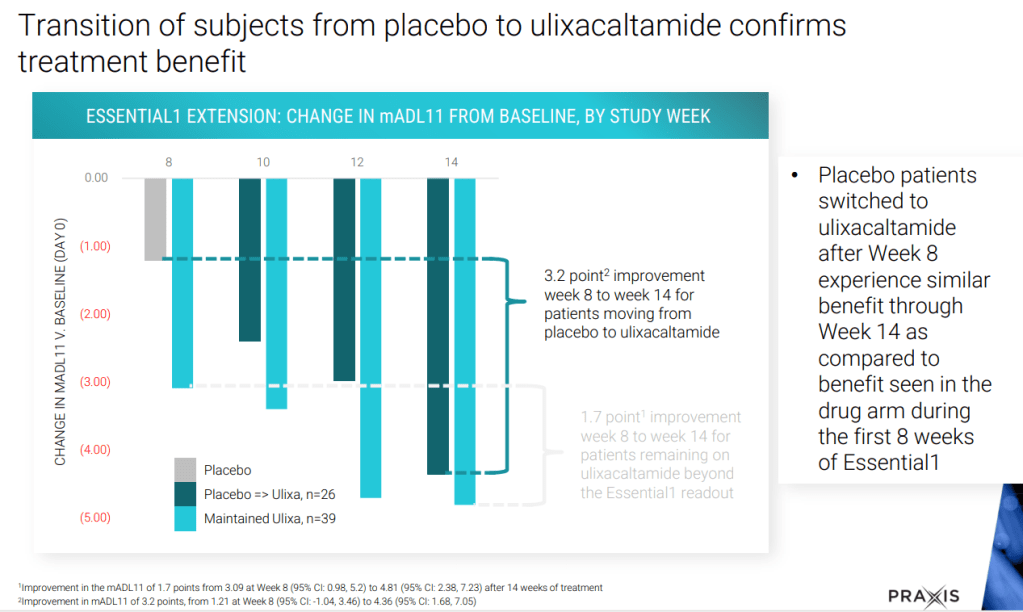
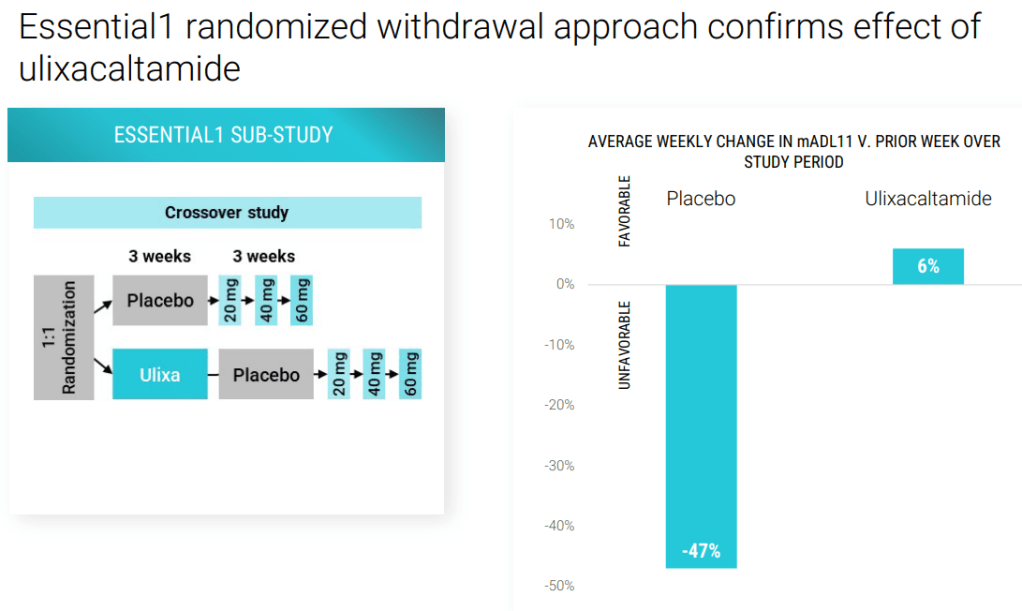
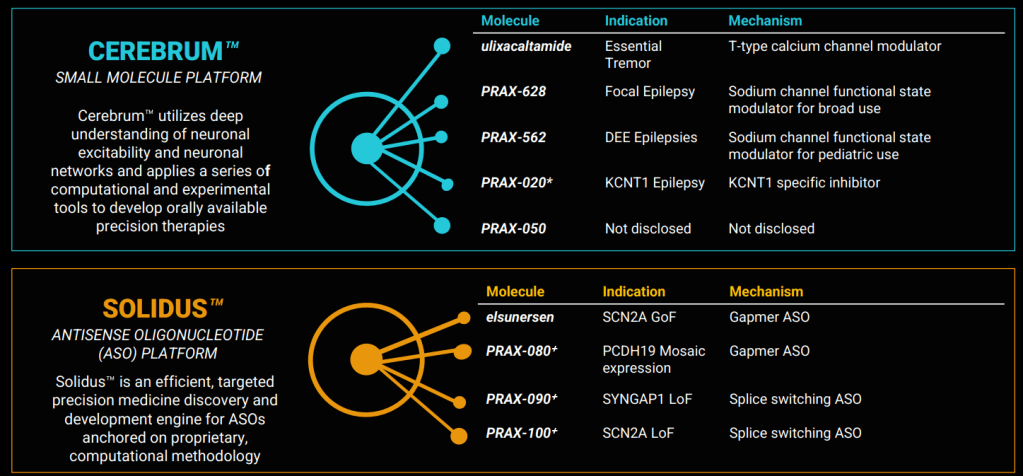
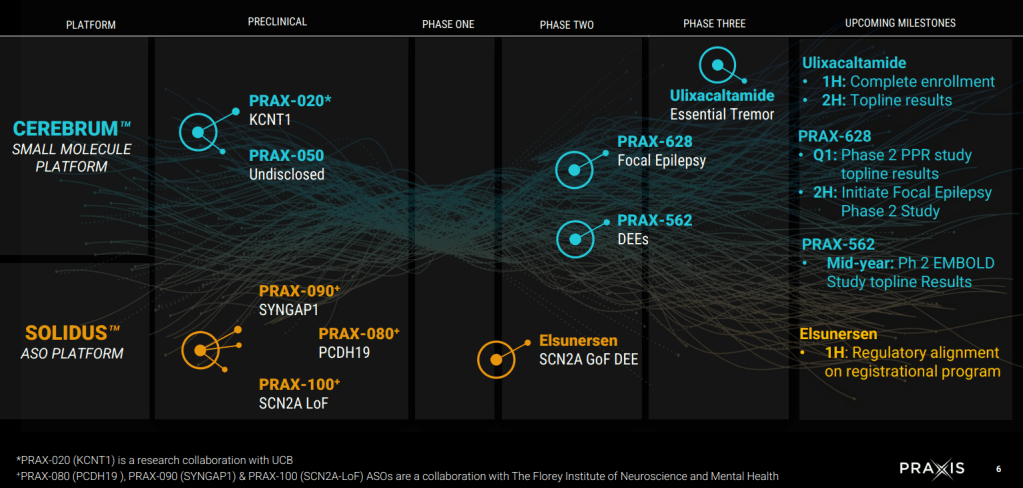
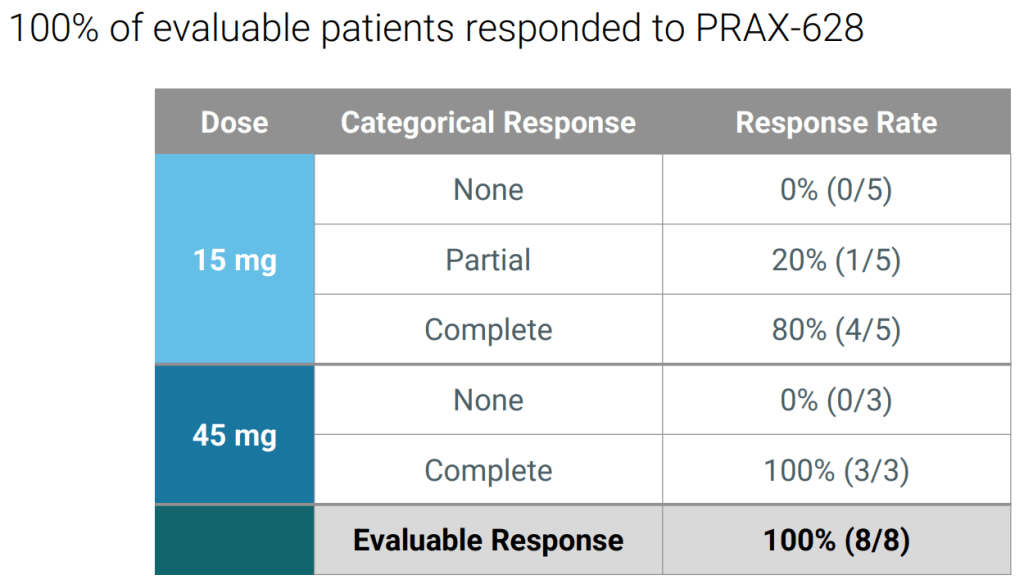
 만약 미국에서 대학을 다녔더라면 어땠을까?")

 Dr. Josep Bassaganya-Riera’s LANCL-Targeting Autoimmune Drug Discovery – from Landos Biopharma to NImmune Biopharma")

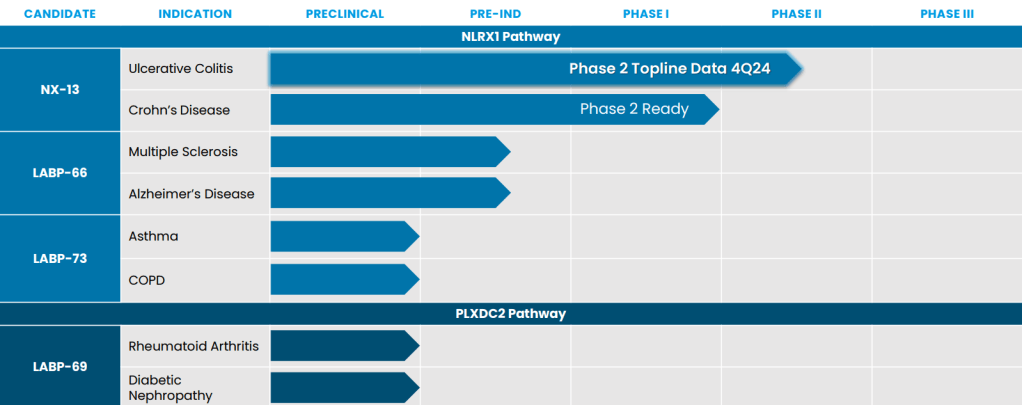
 Merck – Should You Start a Chemistry Podcast?")